Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access
Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc
Journal website http://www.gastrores.org
Case Report
Volume 10, Number 3, June 2017, pages 196-198
Cronkhite-Canada Syndrome: A Rare Cause of Chronic Diarrhea
Umair Iqbala, c, Ahmad Chaudharya, Muhammad Arsalan Karimb, Hafsa Anwarb, Nancy Merrella
aBassett Medical Center, Cooperstown, NY, USA bDow University of Health and Sciences, Karachi, Pakistan cCorresponding Author: Umair Iqbal, Bassett Medical Center, Cooperstown, NY, USA
Manuscript submitted March 06, 2017, accepted April 03, 2017 Short title: Cronkhite-Canada Syndrome doi: https://doi.org/10.14740/gr820w
Cronkhite-Canada syndrome (CCS) is a rare non-hereditary disease characterized by chronic diarrhea, diffuse intestinal polyposis and onychodystrophy. We present here a case of a middle-aged female who presented with chronic intermittent bloody diarrhea associated alopecia and loss of finger and toe nails. Labs were remarkable for microcytic anemia and severe hypoalbuminemia. Endoscopy showed numerous polyps scattered throughout the colon. She was treated with nutritional support and corticosteroid with complete resolution of her symptoms and endoscopic findings. CCS is associated with high mortality and gastrointestinal malignancies. Clinicians should consider CCS in a patient with unexplained chronic diarrhea and ectodermal abnormalities.
Cronkhite-Canada syndrome (CCS) is a rare disease characterized by chronic diarrhea, weight loss, protein-losing enteropathy, malnutrition and ectodermal abnormalities [1]. It is associated with gastrointestinal (GI) malignancies and high mortality [1, 2]. Early diagnosis is important as early application of nutritional therapy can prevent morality associated with this serious disease. We report here a case of CCS in a middle-aged female with successful management.
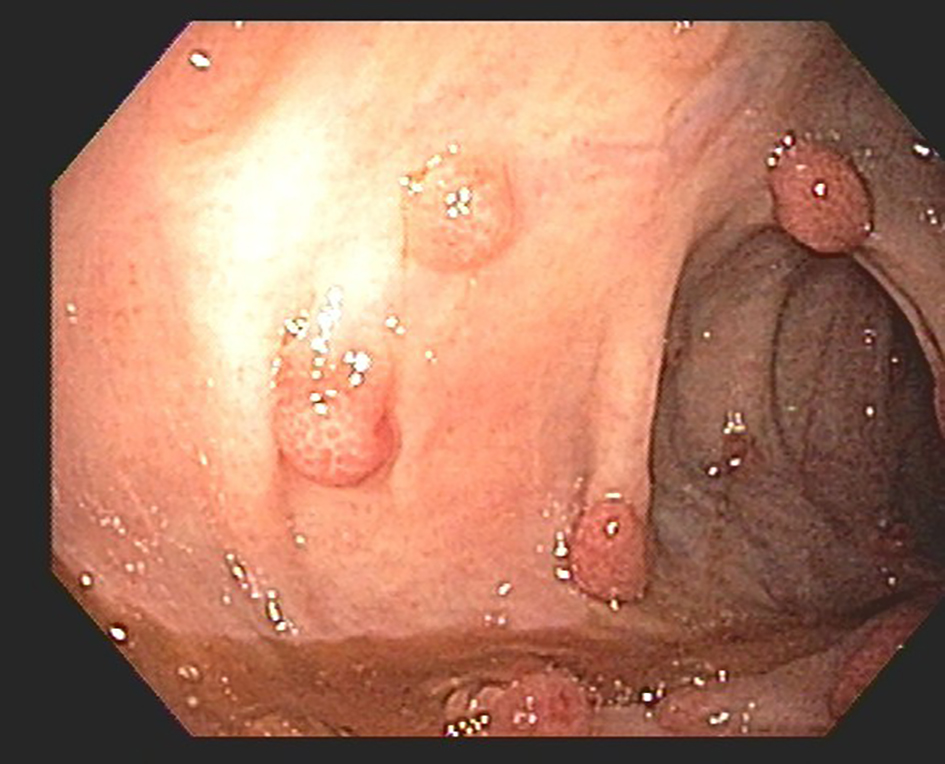
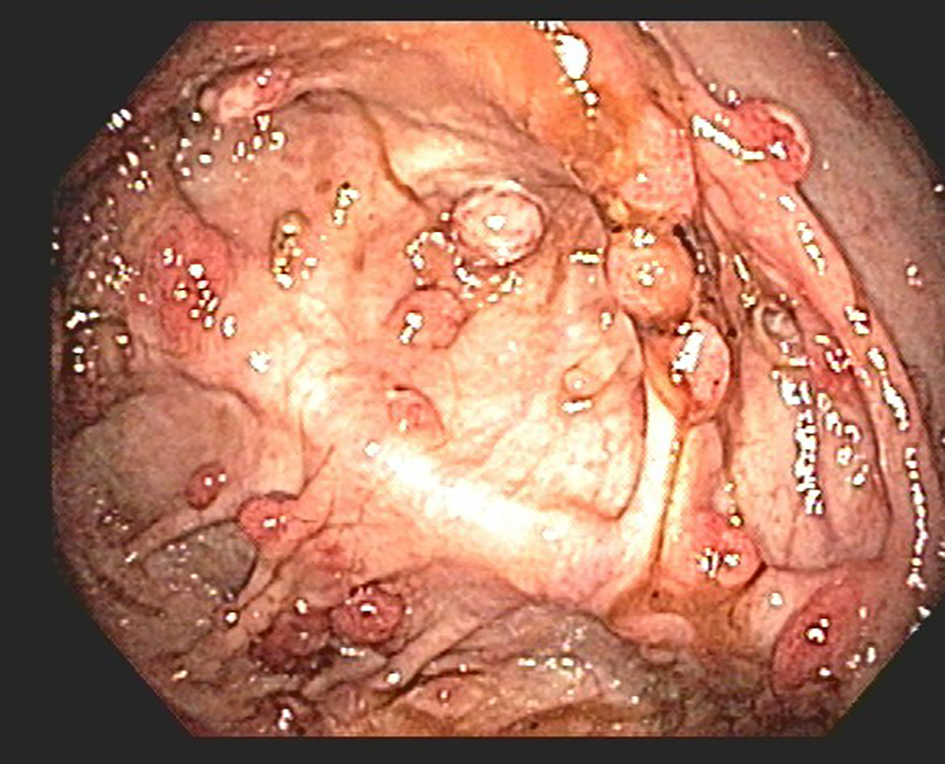
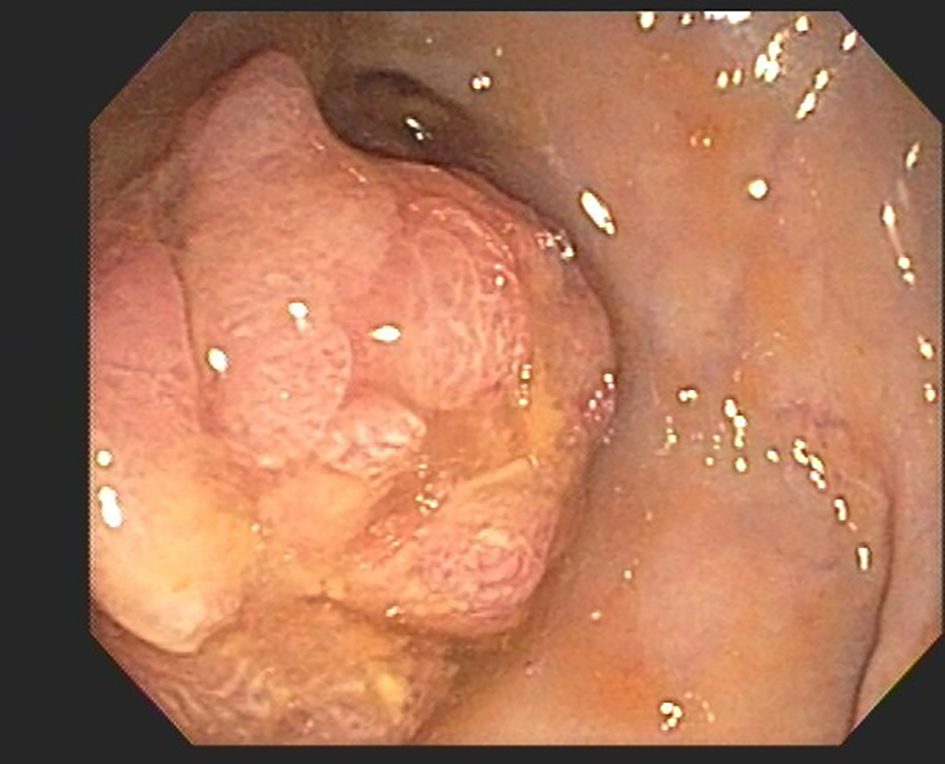
A 55-year-old Korean female with a history of hypothyroidism presented with complaints of chronic intermittent bloody diarrhea, nausea, abdominal pain and weight loss for 2 months. Associated symptoms were alopecia and loss of finger and toenails. She also reported loss of taste sensation. Physical examination showed onychodystrophy and loss of finger and toenails. Physical exam also showed bilateral symmetric edema in lower extremities. Labs showed albumin 1.2 g/dL, INR 1.4 and hematocrit of 24.3 with normal liver and serum chemistries. Stool culture, ova and parasites were negative. EGD revealed extensive gastro-duodenitis with gastric biopsy showing edema and marked mucosal hyperplasia and small bowel biopsy showing inflammation and blunting of the villi. On colonoscopy, innumerous polyps were seen scattered throughout the colon (Figs. 1 and 2). It also showed 45 cm big polyp in a sigmoid colon (Fig. 3). Biopsy showed polyps to be inflammatory with adenomatous change. The clinical, endoscopic and histopathological findings favored the diagnosis of CCS. She was treated with total parenteral nutrition along with corticosteroids and had complete resolution of her cutaneous symptoms and colonoscopic findings. Corticosteroids were then gradually tapered down and azathioprine was added. She is now in remission for 5 years on azathioprine and budesonide.
CCS is a rare non-inherited disorder with incidence of one in a million [3], first reported in 1955 by Leonard Cronkhite and Wilma Canada in two females [4]. Since then more than 500 cases have been described in the literature of this disease [5]. Although cases have been reported worldwide, the majority are from Japan [6]. CCS is more prevalent in males than females with 3:2 ratio and commonly occurs in fifth decade of life with mean age of onset between 50 and 60 years [7]. The pathogenesis of CCS is still unclear; however, in reported cases, it can be associated with systemic lupus erythematosus, vitiligo, rheumatoid arthritis and hypothyroidism suggesting an autoimmune trigger [1, 8].
CCS symptoms include nausea, vomiting, diarrhea, abdominal pain, weight loss, dysgeusia or ageusia. Cutaneous abnormalities associated with CCS include alopecia, onychodystrophy/onycholysis and skin hyperpigmentation [8]. Hyperpigmentation is usually found in neck, face, palms and soles. Skin and nail changes are thought to be secondary to malabsorption and usually follow GI symptoms, although review of literature showed cases in which ectodermal abnormalities present before GI findings. CCS patients have abnormally low levels of protein, anemia and electrolyte abnormalities secondary to malnutrition and chronic diarrhea [8, 9]. These patients can also have elevated inflammatory markers ESR and CRP.
The diagnosis of CCS is based on a combination of clinical, endoscopic and histopathological findings. Typical finding on endoscopy is diffuse GI polyposis mostly sparing the esophagus. In a case series study conducted on 14 patients at Mayo Clinic, 100% of the patients had polyps in stomach, duodenum, colon and rectum but not in the esophagus [8]. Most of the polyps are hamartomatous but inflammatory, adenomatous and hyperplastic polyps can also be present. Polyps usually show marked foveolar hyperplasia, abundant stromal edema, and mononuclear infiltrate [10]. Infiltration of IgG-4 plasma cells has also been reported in CCS polyps [8]. CCS is associated with increased incidence of GI malignancies. Both gastric and colorectal cancers have high incidence in CCS with sigmoid colon and rectum being the common sites [11]. The incidence of colorectal cancer in CCS is reported to be as high as 15% and therefore annual endoscopic screening is recommended in patients diagnosed with this disorder [12].
Management for CCS patients includes correcting electrolyte abnormalities, nutritional support and corticosteroids. Parenteral nutrition may be preferred to provide temporary bowel rest. Because of the side effects associated with the long-term use, corticosteroids are used either for achieving remission in CCS or as a bridge to introduce immunosuppressants like azathioprine [8]. Review of literature revealed cases successfully managed with anti-TNF α therapy like infliximab [13]. Mesalazine or 5-amino salicylic acid has also been reported to induce marked improvements [14]. Other medications used in these patients include antibiotics and acid suppressive medications. Surgical intervention is reserved for complications of CCS like bowel obstruction, prolapse and malignancy.
Untreated CCS is associated with a high mortality. Five-year mortality secondary to complication can be as high as 55% secondary to complications [1]. Complication of CCS includes GI bleeding, severe cachexia, congestive heart failure, intussusception, osteoporotic fractures and sepsis [9].
Conclusion
Clinicians should consider CCS in patients with unexplained diarrhea and ectodermal abnormalities especially in those of Japanese descent. Diffuse GI inflammatory polyposis sparing the esophagus on endoscopy is a hallmark of the disease. Histological examination of the biopsied polyp and intervening mucosa is helpful as well. Nutritional support and treatment with corticosteroids remain the fundamental therapy. Immunosuppresants are steroid sparing and can prevent relapse of symptoms.
Consent
Witnessed informed consent was taken from the patient to publish case report with images.
Daniel ES, Ludwig SL, Lewin KJ, Ruprecht RM, Rajacich GM, Schwabe AD. The Cronkhite-Canada Syndrome. An analysis of clinical and pathologic features and therapy in 55 patients. Medicine (Baltimore). 1982;61(5):293-309. doi
Katayama Y, Kimura M, Konn M. Cronkhite-Canada syndrome associated with a rectal cancer and adenomatous changes in colonic polyps. Am J Surg Pathol. 1985;9(1):65-71. doipubmed
Goto A. Cronkhite-Canada syndrome: epidemiological study of 110 cases reported in Japan. Nihon Geka Hokan. 1995;64(1):3-14. pubmed
Cronkhite LW, Jr., Canada WJ. Generalized gastrointestinal polyposis; an unusual syndrome of polyposis, pigmentation, alopecia and onychotrophia. N Engl J Med. 1955;252(24):1011-1015. doipubmed
Rubio CA, Bjork J. Cronkhite-Canada syndrome - A Case report. Anticancer Res. 2016;36(8):4215-4217. pubmed
Riegert-Johnson DL, Osborn N, Smyrk T, Boardman LA. Cronkhite-Canada syndrome hamartomatous polyps are infiltrated with IgG4 plasma cells. Digestion. 2007;75(2-3):96-97. doipubmed
Ward EM, Wolfsen HC. Review article: the non-inherited gastrointestinal polyposis syndromes. Aliment Pharmacol Ther. 2002;16(3):333-342. doi
Sweetser S, Ahlquist DA, Osborn NK, Sanderson SO, Smyrk TC, Chari ST, Boardman LA. Clinicopathologic features and treatment outcomes in Cronkhite-Canada syndrome: support for autoimmunity. Dig Dis Sci. 2012;57(2):496-502. doipubmed
Watanabe C, Komoto S, Tomita K, Hokari R, Tanaka M, Hirata I, Hibi T, et al. Endoscopic and clinical evaluation of treatment and prognosis of Cronkhite-Canada syndrome: a Japanese nationwide survey. J Gastroenterol. 2016;51(4):327-336. doipubmed
Brosens LA, Wood LD, Offerhaus GJ, Arnold CA, Lam-Himlin D, Giardiello FM, Montgomery EA. Pathology and Genetics of Syndromic Gastric Polyps. Int J Surg Pathol. 2016;24(3):185-199. doipubmed
Yashiro M, Kobayashi H, Kubo N, Nishiguchi Y, Wakasa K, Hirakawa K. Cronkhite-Canada syndrome containing colon cancer and serrated adenoma lesions. Digestion. 2004;69(1):57-62. doipubmed
Nagata K, Sato Y, Endo S, Kudo SE, Kushihashi T, Umesato K. CT endoscopy for the follow-up of Cronkhite-Canada syndrome. Int J Colorectal Dis. 2007;22(9):1131-1132. doipubmed
Boland BS, Bagi P, Valasek MA, Chang JT, Bustamante R, Madlensky L, Sandborn WJ, et al. Cronkhite Canada Syndrome: Significant Response to Infliximab and a Possible Clue to Pathogenesis. Am J Gastroenterol. 2016;111(5):746-748. doipubmed
Takakura M, Adachi H, Tsuchihashi N, Miyazaki E, Yoshioka Y, Yoshida K, Oryo F, Sawada T. A case of Cronkhite-Canada Syndrome markedly improved with mesalazine therapy. Digestive Endoscopy. 2004;16(1):74-78.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.