

| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website https://www.gastrores.org |
Original Article
Volume 17, Number 3, June 2024, pages 126-132

Analysis of Efficacy and Safety of Laparoscopy Plus Choledochoscopy Combined With Holmium Laser Lithotripsy for Choledocholithiasis and Hepatolithiasis
Hui Lia, Qun Feng Zhongb, d, Qiong Rong Liua, Qiang Wua, Wen Zhanga, Guo Pei Luoc
aDepartment of General Surgery, Xingguo Hospital Affiliated to Gannan Medical College, Jiangxi 342400, China
bDepartment of Ultrasound Medicine, Xingguo Hospital Affiliated to Gannan Medical College, Jiangxi 342400, China
cDepartment of Pancreatic Surgery, Affiliated Cancer Hospital of Fudan University, Shanghai 200000, China
dCorresponding Author: Qun Feng Zhong, Department of Ultrasound Medicine, Xingguo Hospital Affiliated to Gannan Medical College, Jiangxi 342400, China
Manuscript submitted March 4, 2024, accepted April 29, 2024, published online June 29, 2024
Short title: Laparoscopy, Choledochoscopy and HLL in Biliary Stone
doi: https://doi.org/10.14740/gr1710
| Abstract | ▴Top |
Background: With the advancement of laparoscopic technology, the combination of laparoscopy, choledochoscopy, and holmium laser lithotripsy has emerged as an effective treatment modality for both choledocholithiasis and hepatolithiasis. This study aimed to assess the efficacy and safety of this approach.
Methods: Retrospective analysis was conducted on the medical records of 76 patients diagnosed with choledocholithiasis and hepatolithiasis between April 2021 and March 2023. Patients were divided into two groups based on the treatment plan: the control group, which underwent traditional laparotomy and choledochoscopy lithotripsy (n = 38), and the experimental group, which underwent laparoscopy combined with choledochoscopy and holmium laser lithotripsy (n = 38). Comparative analysis was performed on various operation-related parameters, stone-free rate, complication rates, and changes in biochemical, liver function, inflammatory, stress response indicators, and pain scores between the two groups.
Results: The experimental group demonstrated significantly shorter stone removal time, reduced intraoperative bleeding, and shorter hospital stay compared to the control group (P < 0.05). Moreover, the experimental group exhibited lower incidence of postoperative complications and lower pain scores at 2 weeks to 3 months post-operation (P < 0.05). Biochemical indicators including total bile acid (TBA), total bilirubin (TBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and glutamyl transpeptidase (GGT) were significantly lower in the observation group compared to the control group (P < 0.05). Additionally, stress and inflammation indicators were also lower in the experimental group (P < 0.05).
Conclusions: The combination of laparoscopy, choledochoscopy, and holmium laser lithotripsy presents favorable therapeutic outcomes in the management of choledocholithiasis and hepatolithiasis, indicating its potential for widespread clinical application.
Keywords: Laparoscopy; Choledochoscopy; Holmium laser lithotripsy; Choledocholithiasis and hepatolithiasis; Safety; Bile biochemistry; Stress response
| Introduction | ▴Top |
Bile duct lithiasis, including both extrahepatic and intrahepatic types (choledocholithiasis and hepatolithiasis, respectively), is notably prevalent in clinical hepatobiliary surgery. Main clinical manifestations include epigastric pain, jaundice, and fever, among others. This condition is characterized by a high incidence and recurrence rate, with severe cases posing a threat to patient safety [1]. Traditional treatments like drug therapy, cholangiography, and surgery, particularly laparotomy, have been standard, though they often lead to large wounds and longer recovery times [2-5]. With advancements in medical technology, laparoscopic minimally invasive surgery is becoming more common [6]. Newer methods such as laparoscopy combined with choledochoscopy and holmium laser lithotripsy are proving effective in reducing surgery time, intraoperative bleeding, postoperative pain, and liver function damage, while also improving stone clearance rates [7-11]. This study aimed to evaluate the clinical efficacy of these combined approaches in treating bile duct lithiasis, assessing outcomes such as liver function, inflammation, stress, and postoperative complications and pain.
| Materials and Methods | ▴Top |
A total of 76 patients diagnosed with intrahepatic and extrahepatic bile duct lithiasis who were admitted to our hospital from April 2021 to March 2022, were enrolled in this study. The patients were divided into two groups based on the surgical interventions: the control group which underwent traditional laparotomy and choledochoscopy lithotripsy (n = 38), and the experimental group which underwent laparoscopy combined with choledochoscopy and holmium laser lithotripsy. Retrospective analysis of the medical records showed no significant differences between the two groups (Table 1).
 Click to view | Table 1. Clinical Characteristics of Patients |
The study included patients diagnosed with bile duct lithiasis confirmed by ultrasound or computed tomography (CT), with a bile duct diameter over 1 cm. Additionally, adherence to diagnostic criteria outlined in the “Guidelines for the Diagnosis and Therapy of Hepatobiliary Stones” was required. Patients who had difficult to locate stones or unsuitable for extracorporeal lithotripsy were included. Exclusion criteria comprised suspicion of gallbladder or cholangiocarcinoma, presence of liver cirrhosis, portal hypertension, or varicose veins, abnormal coagulation function, prior biliary tract surgery, or autoimmune diseases/severe organic diseases.
The study was approved by the Ethical Committee of Xingguo Hospital Affiliated to Gannan Medical College (20210401) and was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
Methods
In the control group, all subjects underwent laparotomy and choledochoscopy for stone removal, following standard draping and disinfection protocols.
In the experimental group, subjects underwent laparoscopy combined with choledochoscopy and holmium laser lithotripsy.
Observation indicators
The operation-related indicators (time of stone removal, blood loss, length of stay) and stone removal outcomes of the patients included in the analysis were meticulously examined.
The frequency of related complications, including biliary fistula, incision infection, fever, and biliary tract bleeding, during the patients’ recovery process was meticulously documented between the groups.
For blood chemical tests and liver function assessment, fasting venous blood samples (5 mL) were collected both before and 1 week after the operation. After centrifugation at 3,000 r/min for 10 min, levels of total bile acid (TBA), total bilirubin (TBIL) alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and glutamyl transpeptidase (GGT) were determined using an automatic biochemical analyzer.
To evaluate the levels of inflammatory and stress-related markers, venous blood samples (6 mL) were collected from patients before and 3 days post-surgery. Serum levels of epinephrine (EP) and cortisol (Cor) were determined by chemiluminescence immunoassay. Levels of C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α) were determined by enzyme-linked immunosorbent assay, while neutrophil count (NEUT) levels were measured by an automatic hematology analyzer.
Pain scores were measured using the digital analog scoring method immediately after the operation, as well as at 2 weeks, 4 weeks, and 3 months post-operation.
Statistics
The data were analyzed using SPSS 21.0 statistical software. Independent samples t-test was utilized for numeric variables, while the Chi-square test was employed for categorical variables. P < 0.05 indicated statistical significance.
| Results | ▴Top |
Comparison of surgery-related indicators and stone clearance rate
The control group had a significantly longer stone extraction time (5.95 ± 0.23 vs. 4.05 ± 0.23, P = 0.001) (Table 2). In addition, blood bleeding was also more in the control group, compared with the experimental group (70.34 ± 6.27 vs. 44.84 ± 3.38, P = 0.001) (Table 2). The length of hospital stay in the experimental group was shorter than the control group (9.16 ± 0.68 vs. 6.95 ± 0.46, P = 0.001) (Table 2). In terms of stone clearance, the experimental group showed a significantly higher rate than the control group (68.42% vs. 92.11%, P = 0.009) (Table 2).
Click to view | Table 2. Analysis of Surgery-Related Indicators and Stone Clearance Rate |
Analysis of treatment-related complications
The complications evaluated include biliary fistula, incision infection, fever, and biliary hemorrhage. The statistical analysis indicated a significant difference between the two groups (P = 0.025), suggesting that the experimental group had significantly fewer complications compared to the control group (Table 3).
Click to view | Table 3. Analysis of Treatment-Related Complications |
Analysis of bile biochemical index
Changes in bile biochemical index levels between pre-operation and 1 week after surgery, specifically TBA and TBIL were evaluated.
For the control group, the preoperative TBA level dropped from 83.08 to 33.29 µmol/L, while the experimental group showed a more profound decrease from 83.24 to 9.87 µmol/L (Fig. 1a). The reduction of TBIL level in the experimental group was also pronounced than the control group (Fig. 1b).
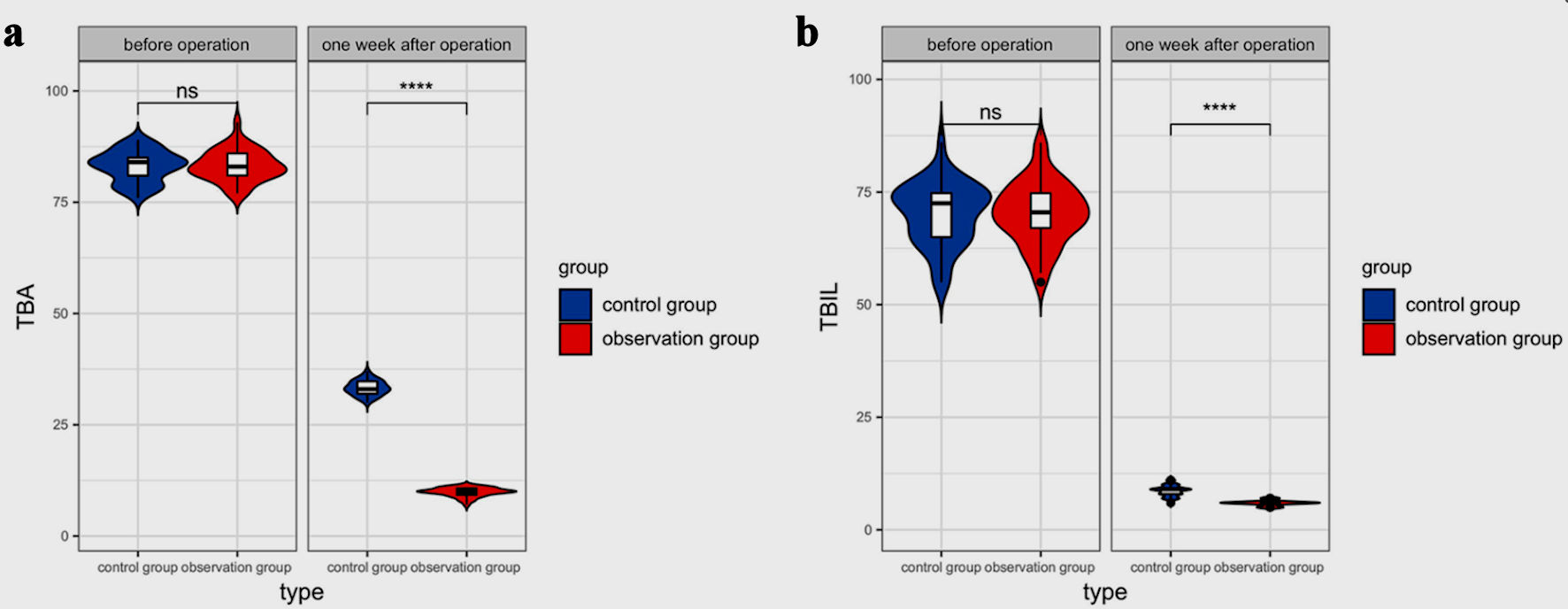 Click for large image | Figure 1. Analysis of bile biochemical index levels among groups. TBA (a) and TBIL (b) levels in patients before and 1-week post-surgery. ****P < 0.0001, ns: not significant. TBA: total bile acid; TBIL: total bilirubin. |
Analysis of liver function index levels
We also conducted detailed comparison of liver function index levels, specifically ALT, AST, ALP, and GGT between two groups of patients. At the outset, both the control and observation groups had nearly identical liver function index levels of ALT, AST, ALP, and GGT. However, 1 week after surgery, the experimental group exhibited significantly greater improvements across all indices compared to the control group (Fig. 2).
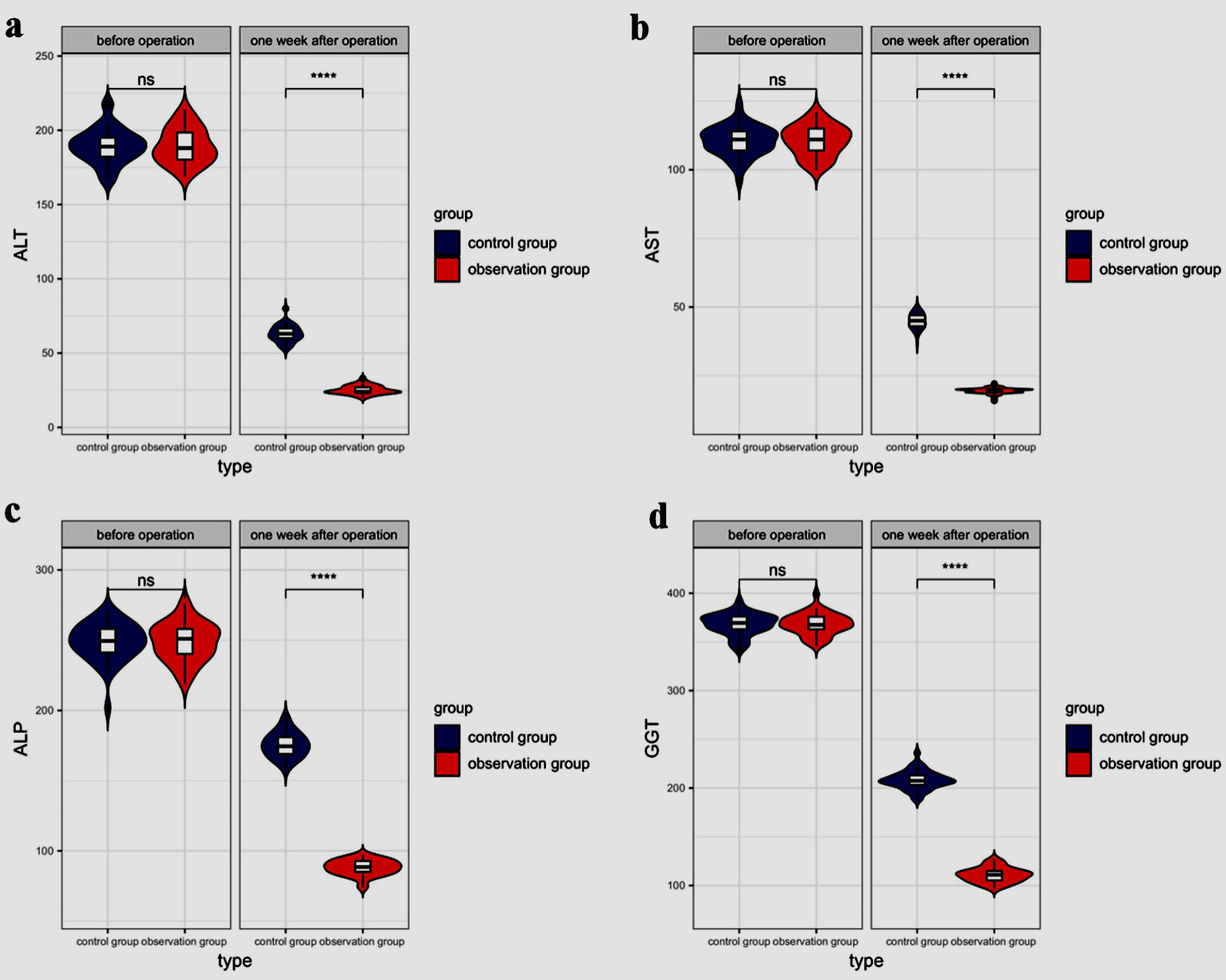 Click for large image | Figure 2. Analysis of liver function indicators between groups. Levels of ALT (a), AST (b), ALP (c), GGT (d) in patients from the control and experimental group before and after surgery. ****P < 0.0001, ns: not significant. ALT: alanine aminotransferase; AST: aspartate aminotransferase; ALP: alkaline phosphatase; GGT: glutamyl transpeptidase. |
Analysis of inflammatory index levels
Changes in inflammatory index levels, specifically CRP, IL-6, and TNF-α in the control group and the experimental group were measured preoperatively and 3 days post-surgery. There was no difference of the baseline levels of CRP, IL-6 and TNF-α in both groups, while their levels were significantly lower in the experimental group at 3 days post-surgery (Fig. 3).
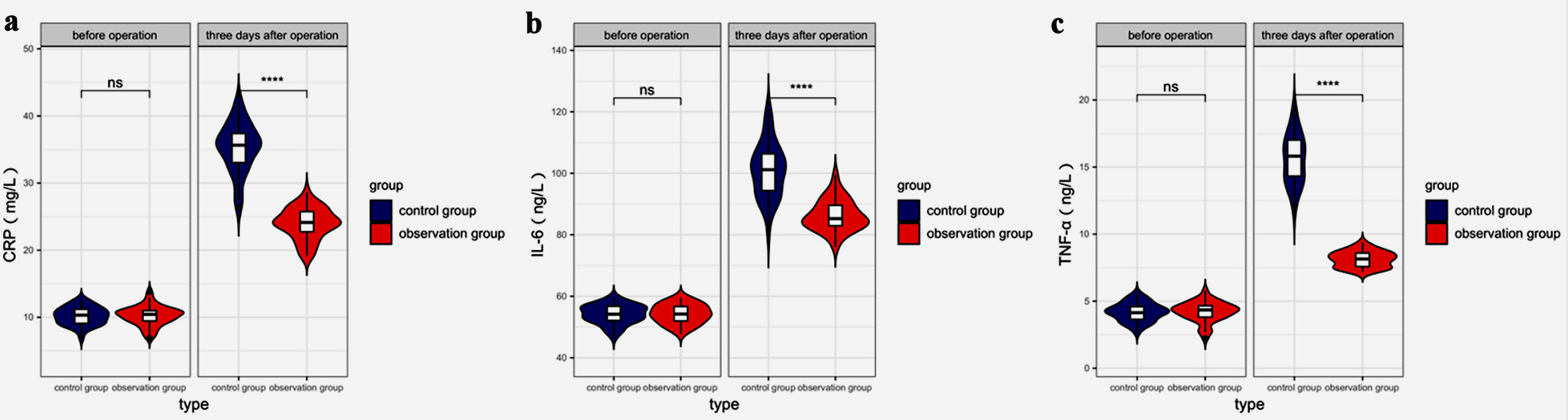 Click for large image | Figure 3. Analysis of inflammatory index levels between groups. Levels of CRP (a), IL-6 (b), and TNF-α (c) in patients from the control and experimental group before and 3 days after surgery. ****P < 0.0001, ns: not significant. CRP: C-reactive protein; IL-6: interleukin-6; TNF-α: tumor necrosis factor-α. |
Analysis of stress response
Next, we evaluated the stress response index including Cor, neutrophil percentage, and EP both pre-operation and 3 days post-surgery. No significant difference was observed in these two groups before surgery, while the post-surgery levels of Cor, NEUT, and EP were significantly lower in the experimental group (Figure 4).
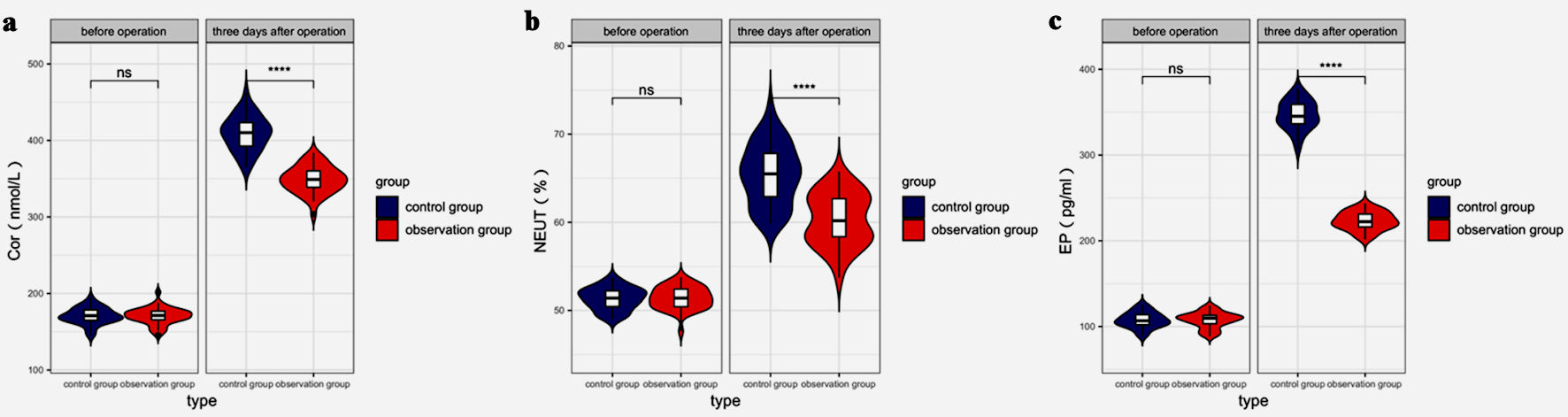 Click for large image | Figure 4. Analysis of stress response index levels between groups. Levels of Cor (a), NEUT (b), and EP (c) in patients from the control and experimental group before and 3 days after surgery. ****P < 0.0001, ns: not significant. Cor: cortisol; EP: epinephrine; NEUT: neutrophil count. |
Analysis of pain levels
Pain levels in patients suffering between two groups of 38 patients were evaluated at various time points following surgery: immediately after surgery, 2-week, 4-week, and 3-month post-procedure. There was no difference of pain levels in the two groups after surgery, but it became significantly lower since 2 weeks post-operation (Table 4).
Click to view | Table 4. Analysis of Pain Score |
| Discussion | ▴Top |
The complexity of managing intrahepatic and extrahepatic bile duct stones, due to the intricate nature of pathological changes and the narrowness of bile ducts, poses a significant challenge in achieving complete stone removal in a single session, with clinical evidence pointing towards a high rate of postoperative residual stones and the need for repeat surgeries in a substantial fraction of cases [12, 13]. Historically, laparotomy was the primary treatment for bile duct lithiasis but was less effective for large or incarcerated stones, leading to longer surgery times and increased risks [14, 15]. The shift to minimally invasive techniques such as laparoscopy combined with choledochoscopy and holmium laser lithotripsy has reduced trauma, complications, and promoted faster recovery [16, 17]. Holmium laser lithotripsy enhances stone removal and success rates [18, 19]. It reduces blood loss and improves recovery, making the surgery less physically and psychologically impactful [20]. Studies show that laparoscopic and choledochoscopic holmium laser lithotripsy leads to better outcomes in terms of surgery duration, hospital stay, bleeding, pain scores, and complication rates from 2 weeks to 3 months post-surgery, aligning with previous findings [21-25].
Our study also evaluated liver function biochemical markers, revealing significant improvements in the observation group compared to the control group postoperatively. This underscores the efficacy of the integrated surgical approach in managing bile duct lithiasis and enhancing liver function, contributing to a clearer operative field and improved liver environment.
The study found that the minimally invasive approach significantly reduces postoperative stress and inflammation by lowering EP and Cor levels [26-28]. This is attributed to the surgery’s precise and minimally disruptive nature. In conclusion, combining laparoscopy, choledochoscopy, and holmium laser lithotripsy offers a less invasive and effective treatment for bile duct lithiasis, enhancing liver function and reducing surgical stress.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received for this study.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Informed consent was obtained from all participants.
Author Contributions
Study conception and design: QZ; data collection: HL, QL, QW, and WZ; analysis and interpretation of results: HL, QZ, QL, and GL; draft manuscript preparation: HL, QL and QW; manuscript editing and revision: QZ. All authors reviewed the results and approved the final version of the manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Davrieux CF, Palermo M, Houghton E, Serra E, Acquafresca P, Finger C, Alvear Castro D, et al. Image-guided surgery for common bile duct stones after Roux-en-Y gastric bypass. J Laparoendosc Adv Surg Tech A. 2021;31(2):176-182.
doi pubmed - Liu YY, Li TY, Wu SD, Fan Y. The safety and feasibility of laparoscopic approach for the management of intrahepatic and extrahepatic bile duct stones in patients with prior biliary tract surgical interventions. Sci Rep. 2022;12(1):14487.
doi pubmed pmc - Geers J, Jaekers J, Topal H, Collignon A, Topal B. Bile duct injury in laparoscopic cholecystectomy with a posterior infundibular approach. International Journal of Hepatobiliary and Pancreatic Diseases. 2022;12(2):13-21.
- Zhang LF, Hou CS, Xu Z, Wang LX, Ling XF, Wang G, Cui L, et al. [Clinical effect of laparoscopic transcystic drainage combined with common bile duct exploration for the patients with difficult biliary stones]. Beijing Da Xue Xue Bao Yi Xue Ban. 2022;54(6):1185-1189.
doi pubmed pmc - Yamaguchi K, Chijiiwa K, Saiki S, Nishihara K, Takashima M, Kawakami K, Tanaka M. Retrospective analysis of 70 operations for gallbladder carcinoma. Br J Surg. 1997;84(2):200-204.
pubmed - Jiang Y, Lu J, Li W, Zhang J, Li L. Primary closure after laparoscopic common bile duct exploration is safe and feasible for patients with non-severe acute cholangitis. Langenbecks Arch Surg. 2022;407(4):1553-1560.
doi pubmed - Tracy BM, Paterson CW, Kwon E, Mlaver E, Mendoza A, Gaitanidis A, Rattan R, et al. Outcomes of same admission cholecystectomy and endoscopic retrograde cholangiopancreatography for common bile duct stones: A post hoc analysis of an Eastern Association for the Surgery of Trauma multicenter study. J Trauma Acute Care Surg. 2021;90(4):673-679.
doi pubmed - Tracy BM, Paterson CW, Torres DM, Young K, Saxe JM, Kinstedt DP, Zielinski MD, et al. The effect of prolonged antibiotics on postoperative complications for common bile duct stones: A post hoc analysis of an EAST multicenter study. J Trauma Acute Care Surg. 2021;91(1):234-240.
doi pubmed - Amaral AC, Hussain WK, Han S. Cholangioscopy-guided electrohydraulic lithotripsy versus laser lithotripsy for the treatment of choledocholithiasis: a systematic review. Scand J Gastroenterol. 2023;58(10):1213-1220.
doi pubmed - Zhang Z, Yuan H. Strategy of laparoscopy and choledochoscopy or duodenoscopy for the treatment of cholecystolithiasis combined with choledocholithiasis. Chinese Journal of Digestive Surgery. 2015;14(04).
- Jones T, Al Musawi J, Navaratne L, Martinez-Isla A. Holmium laser lithotripsy improves the rate of successful transcystic laparoscopic common bile duct exploration. Langenbecks Arch Surg. 2019;404(8):985-992.
doi pubmed pmc - Neri V, Ambrosi A, Fersini A, Tartaglia N, Lapolla F. Common bile duct lithiasis: therapeutic approach. Ann Ital Chir. 2013;84(4):405-410.
pubmed - Wu Y, Xu CJ, Xu SF. Advances in risk factors for recurrence of common bile duct stones. Int J Med Sci. 2021;18(4):1067-1074.
doi pubmed pmc - Johansson E, Osterberg J, Sverden E, Enochsson L, Sandblom G. Intervention versus surveillance in patients with common bile duct stones detected by intraoperative cholangiography: a population-based registry study. Br J Surg. 2021;108(12):1506-1512.
doi pubmed pmc - Zhen W, Xu-Zhen W, Nan-Tao F, Yong L, Wei-Dong X, Dong-Hui Z. Primary closure versus T-tube drainage following laparoscopic common bile duct exploration in patients with previous biliary surgery. Am Surg. 2021;87(1):50-55.
doi pubmed - Kao CT, Seagar R, Heathcock D, Tacey M, Lai JM, Yong T, Houli N, et al. Factors that predict the success of laparoscopic common bile duct exploration for choledocholithiasis: a 10-year study. Surg Laparosc Endosc Percutan Tech. 2021;31(5):565-570.
doi pubmed - Chae MK, Lee SH, Joo KR. Assessment of the possible risk factors for primary common bile duct stone recurrence after cholecystectomy. Surg Endosc. 2021;35(12):6497-6504.
doi pubmed - Al-Ardah M, Barnett RE, Morris S, Abdelrahman T, Nutt M, Boyce T, Rasheed A. Lessons learnt from the first 200 unselected consecutive cases of laparoscopic exploration of common bile duct stones at a district general hospital. Surg Endosc. 2021;35(11):6268-6277.
doi pubmed - Vu AN, Eskander J, Chan STF, Houli N, Bui HT. Impact of single-stage laparoscopic trans-cystic exploration on hospital procedures, admissions and length-of-stay in common bile duct stone clearance. ANZ J Surg. 2021;91(12):2695-2700.
doi pubmed - Kumar A, Chumber S. Common bile duct dilatation with stones indicates requirement for early drainage in patients with or without cholangitis at AIIMS, New Delhi. Indian Medical Journal. 2020;114(3):17-20.
- Tracy BM, Paterson CW, Torres DM, Young K, Hochman BR, Zielinski MD, Burruss SK, et al. Risk factors for complications after cholecystectomy for common bile duct stones: An EAST multicenter study. Surgery. 2020;168(1):62-66.
doi pubmed - Olausson M, Westen M, Boilesen AEB, Shabanzadeh DM. Laparoscopic common bile duct exploration for common bile duct stones complicated with cholangitis in patients with Roux-en-Y gastric bypass-clinical experience from three cases. Obes Surg. 2020;30(12):5142-5144.
doi pubmed - Chen H, Jorissen R, Walcott J, Nikfarjam M. Incidence and predictors of common bile duct stones in patients with acute cholecystitis: a systematic literature review and meta-analysis. ANZ J Surg. 2020;90(9):1598-1603.
doi pubmed - Gantois D, Goudard Y, Bourgouin S, Pauleau G, de La Villeon B, Balandraud P. One-stage laparoscopic procedure versus two-stage procedure in the management of common bile duct stones in patients aged 75 and more. J Visc Surg. 2020;157(2):99-106.
doi pubmed - Jaboury IA. Size of the cystic duct is another predictor for common bile duct stones in acute cholecystitis. ANZ J Surg. 2021;91(1-2):214-215.
doi pubmed - Prete A, Yan Q, Al-Tarrah K, Akturk HK, Prokop LJ, Alahdab F, Foster MA, et al. The cortisol stress response induced by surgery: A systematic review and meta-analysis. Clin Endocrinol (Oxf). 2018;89(5):554-567.
doi pubmed - Roth-Isigkeit A, Brechmann J, Dibbelt L, Sievers HH, Raasch W, Schmucker P. Persistent endocrine stress response in patients undergoing cardiac surgery. J Endocrinol Invest. 1998;21(1):12-19.
doi pubmed - Aher S, Waknis P, Shah S, Saha A, Bhujbal P, Gupta D. Evaluation of presurgical serum cortisol level in patients undergoing major maxillofacial surgery. Ann Maxillofac Surg. 2020;10(1):25-30.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Gastroenterology Research is published by Elmer Press Inc.