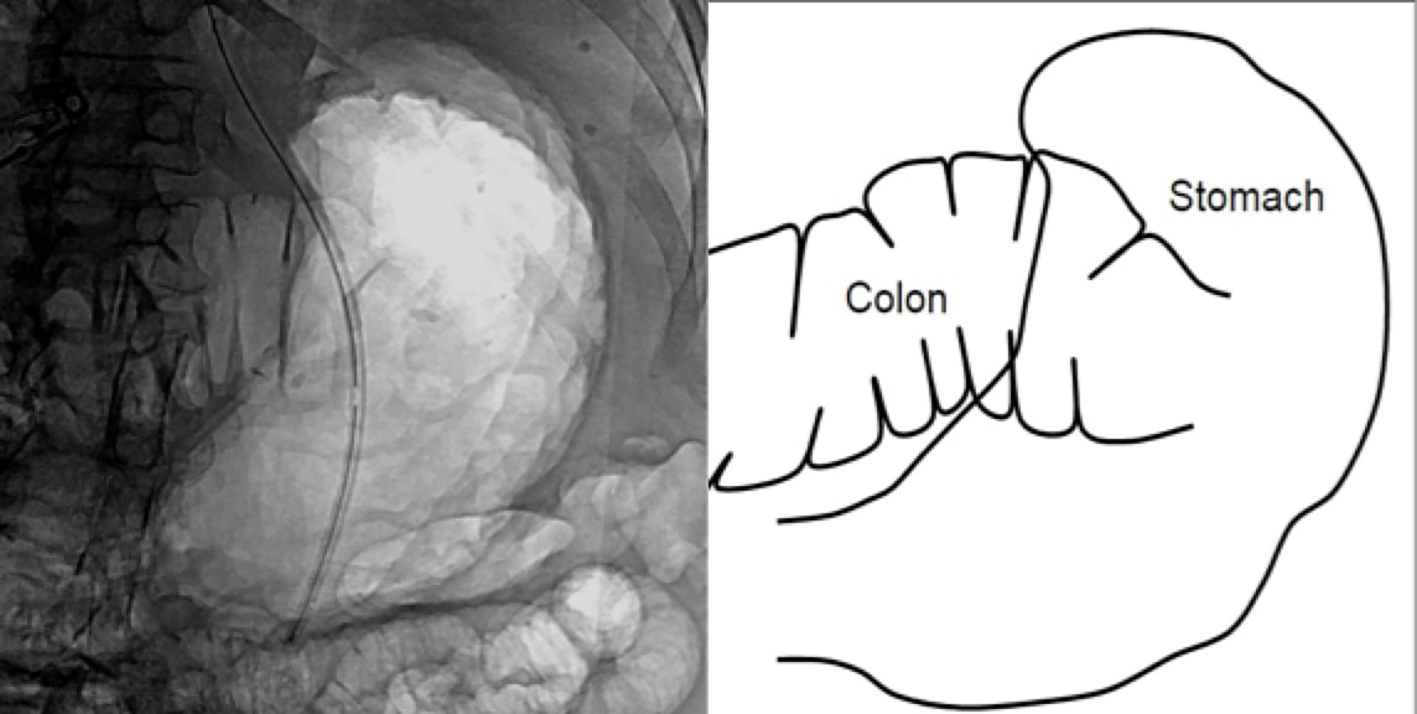
Figure 1. Fluoroscopic evaluation of the abdomen demonstrated an air distended colonic loop anterior to the stomach. Accompanying schematic
| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Case Report
Volume 11, Number 2, April 2018, pages 145-149
Trans-Hepatic Percutaneous Endoscopic Gastrostomy Tube Placement: A Case Report of A Rare Complication and Literature Review
Figures
Table
| Author | Age/sex | Indication | PEG technique | Presentation | Diagnosis | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| Chaer et al (2003) [12] | 78 years/female | Oropharyngeal cancer | Trans illumination (pull technique) | 2.5 months later with concerns for tube malfunction | Contrast radiograph: PEG tube within liver | Laparotomy: removal of PEG tube and placement of new tube | No long term complication |
| Gubler et al (2005) [13] | 59 years/male | Nasopharyngeal cancer | Trans illumination | 1 week later with pain around PEG site | Ultrasound: PEG tube along edge of left liver lobe | 10-day course of analgesics with pain resolution | Asymptomatic at 6 month follow up |
| Gubler et al (2005) [13] | 81 years/female | Esophageal cancer | Trans illumination | 1 week later with abdominal discomfort | Ultrasound: PEG tube along edge of left liver lobe | 3-week course of analgesics with pain resolution | Death at 6 weeks from respiratory failure, unrelated to PEG |
| Wiggins et al (2007) [14] | 61 years/female | Prolonged ventilation requirement | Trans illumination (pull technique) | Abdominal pain and hypotension 8 h after procedure | Computed Tomography: PEG tube in left hepatic lobe, 10.1 cm sub capsular hematoma | Laparotomy: tube removal, repair of liver laceration and insertion of new tube | Death at 3 months from respiratory failure, unrelated to PEG |
| Burke et al (2009) [15] | 33 years/male | Intracranial hemorrhage | Trans illumination | Fevers, chills and transaminitis after 7 weeks of placement | Computed Tomography: PEG tube terminus outside stomach near liver | Antibiotics, Laparotomy: tube removal and closure of gastro-hepatic fistula. | Abscess development a week after laparotomy, drained under sonographic guidance. Long term outcome not mentioned |
| Herta et al (2015) [16] | 44 years/no mention | Hypopharyngeal cancer | Transillumination (pull technique) | 4 days later with abdominal pain | Ultrasound: hepatomegaly, peri-hepatic ascites and PEG tube in left hepatic lobe | PEG removal, closure of gastric insertion site. New PEG tube inserted a week later | No immediate complications. Long term outcome not mentioned |