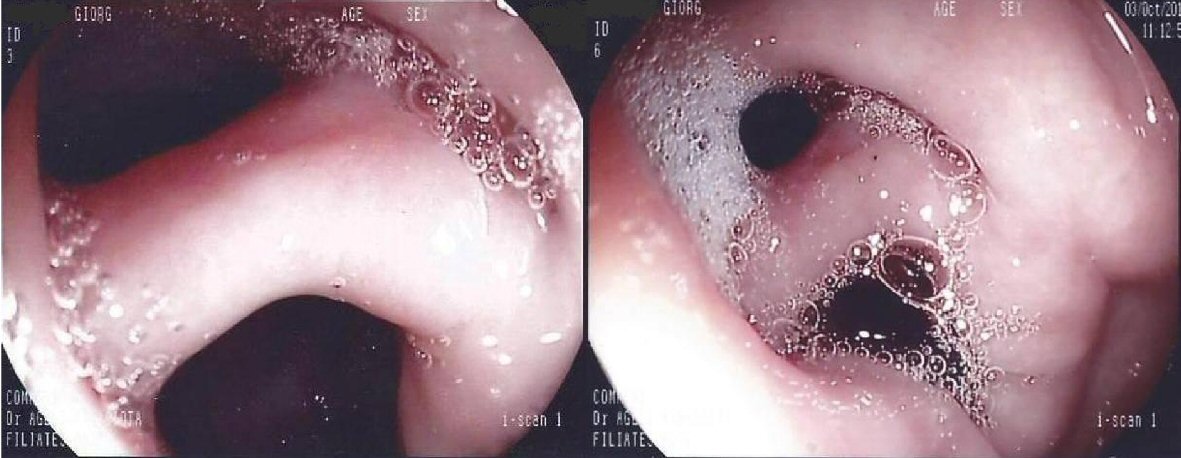
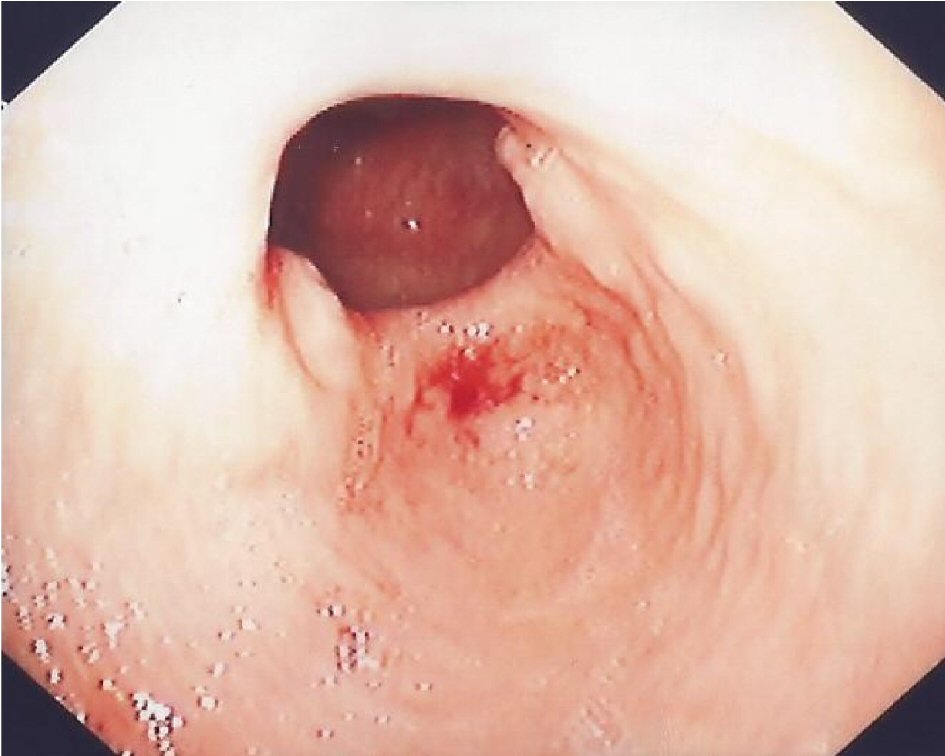
Figure 1. Endoscopic view from the antrum demonstrates double pylorus. The two openings are separated by a bridge from tissue.
| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Case Report
Volume 11, Number 2, April 2018, pages 154-156
Double Pylorus: Report of a Case With Endoscopic Follow-Up and Review of the Literature
Figures
Table
| Incidence | 0.001% to 0.4% of upper gastrointestinal endoscopies |
| Clinical presentation | Chronic upper abdominal pain, dyspepsia, upper gastrointestinal bleeding, vomiting |
| Causes | Gastric ulcer, duodenal ulcer, gastric cancer |
| Risk factors | Ulcerogenic medications, Helicobacter pylori, adrenal adenoma, diabetes mellitus, chronic obstructive disease, chronic renal failure, Behcet’s disease |
| Differential diagnosis | Congenital double pylorus, gastric diverticulum |
| Complications | Gastric outlet obstruction, persistence gastric ulcer |
| Treatment | Endoscopic therapy, surgery |