Figures
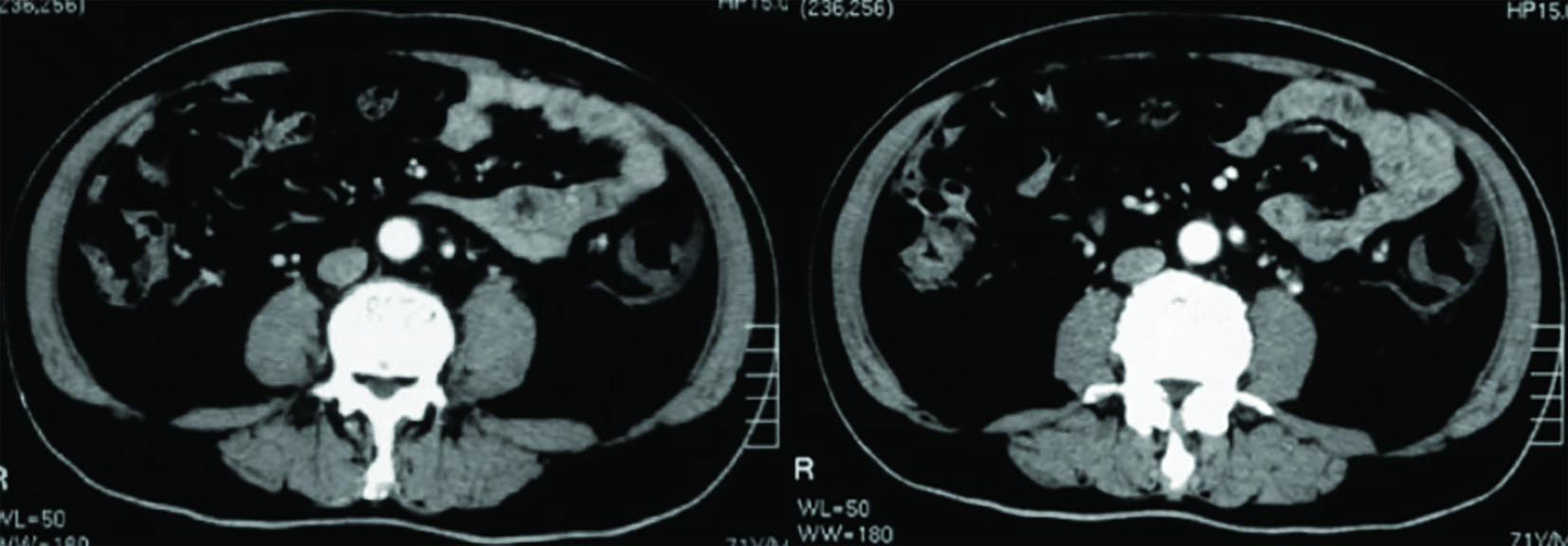
Figure 1. CT imaging of the abdomen showed thickening of the sigmoid colon wall which corresponded to a palpable firm cord-like mass (20 × 5 cm) in the left lower quadrant with tenderness on physical examination.
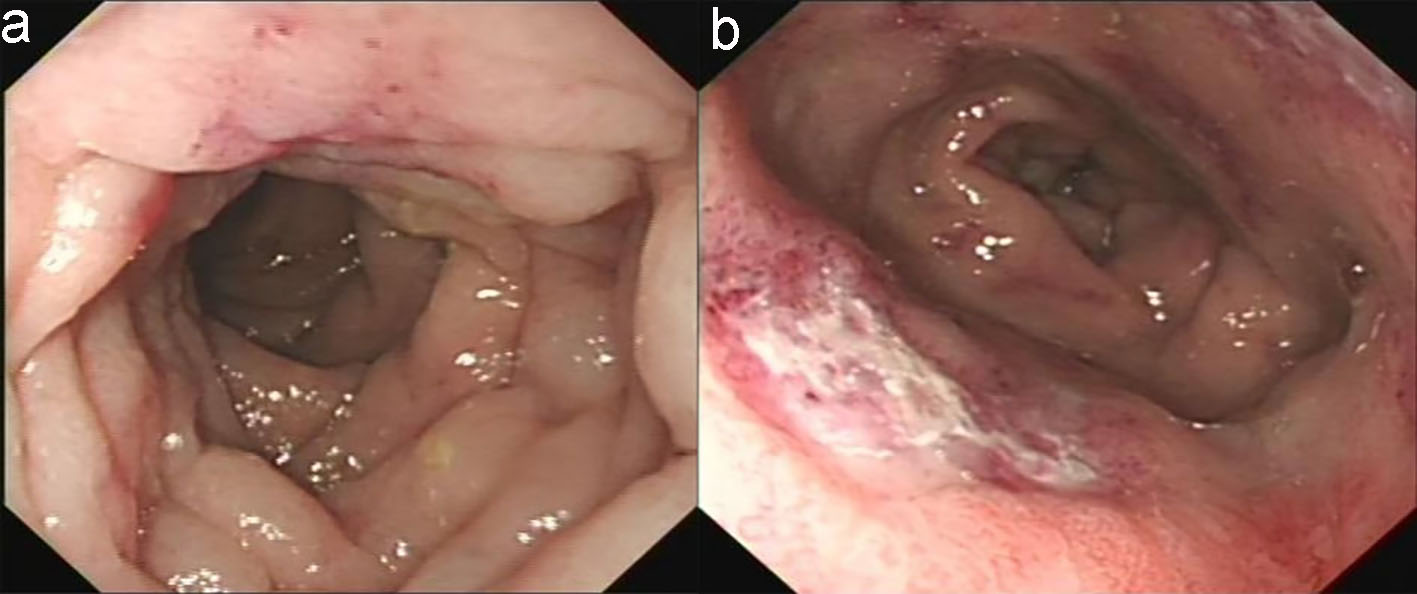
Figure 2. Colonoscopy revealed that the descending colon mucosa had hyperemia, constriction, edema, and with cobble-stone sign (a) and the rectum was the most seriously affected segment which had circumferential erosion and superficial ulcer (b).
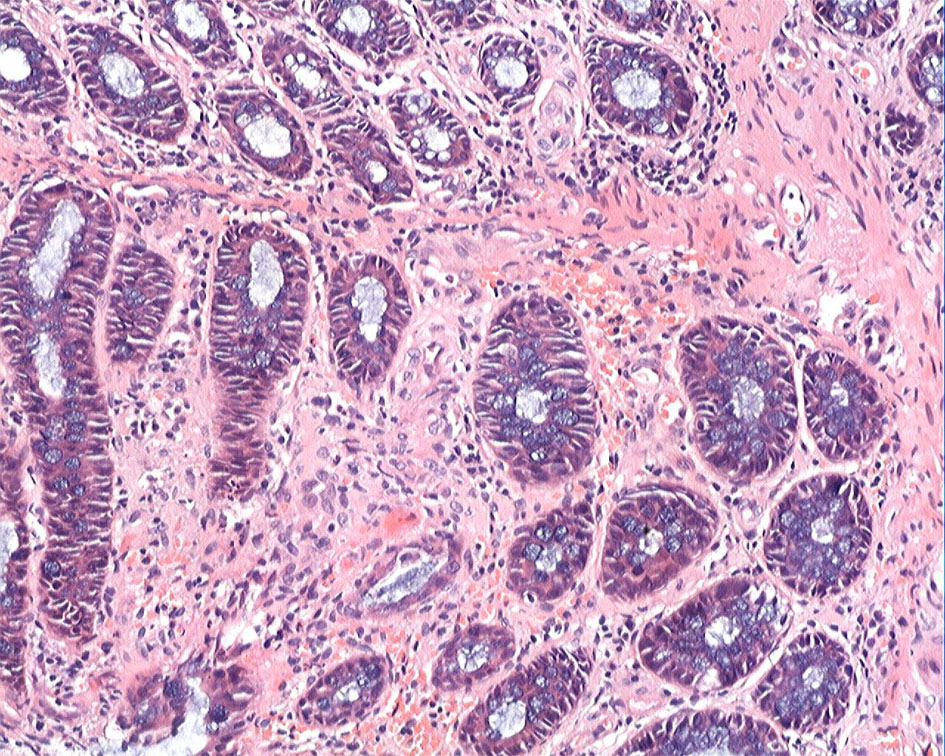
Figure 3. Colonic biopsy demonstrated mucosal infiltration by inflammatory cells and focal interstitial fibrosis (H&E staining, × 20).
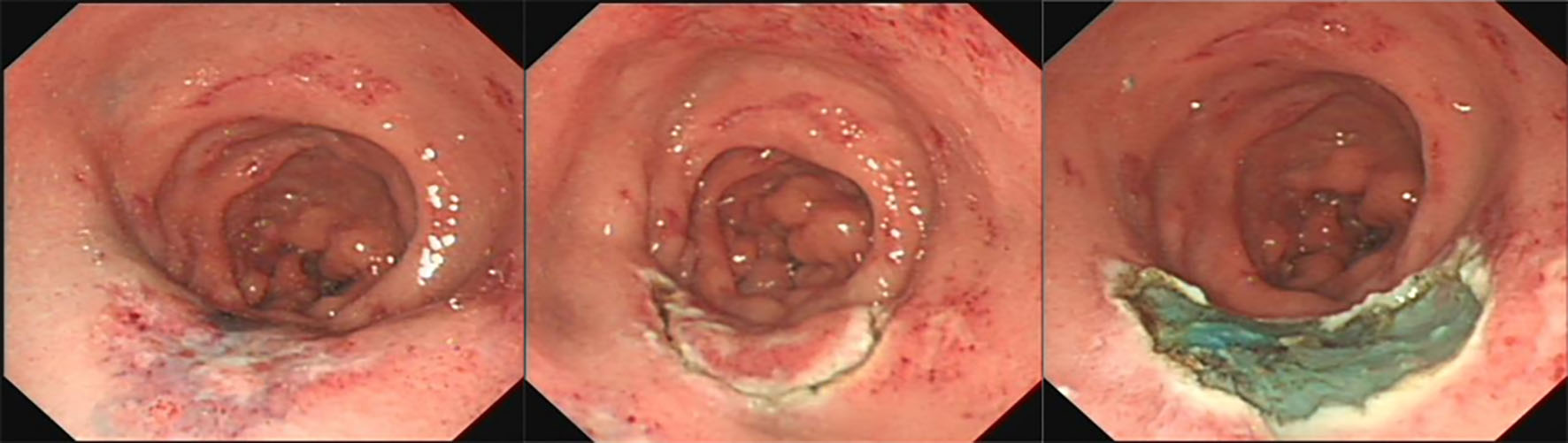
Figure 4. Endoscopic submucosal dissection procedure.
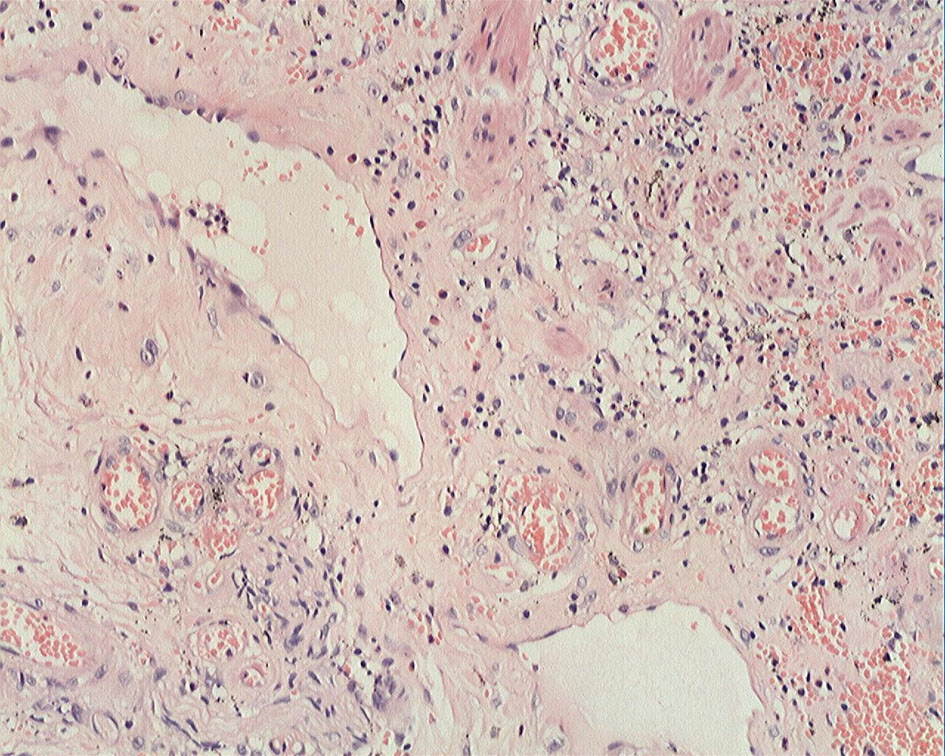
Figure 5. ESD specimen showed erosion, inflammatory exudates, granulation tissue, and fibrinoid degeneration of small blood vessel wall (H&E staining, × 20).
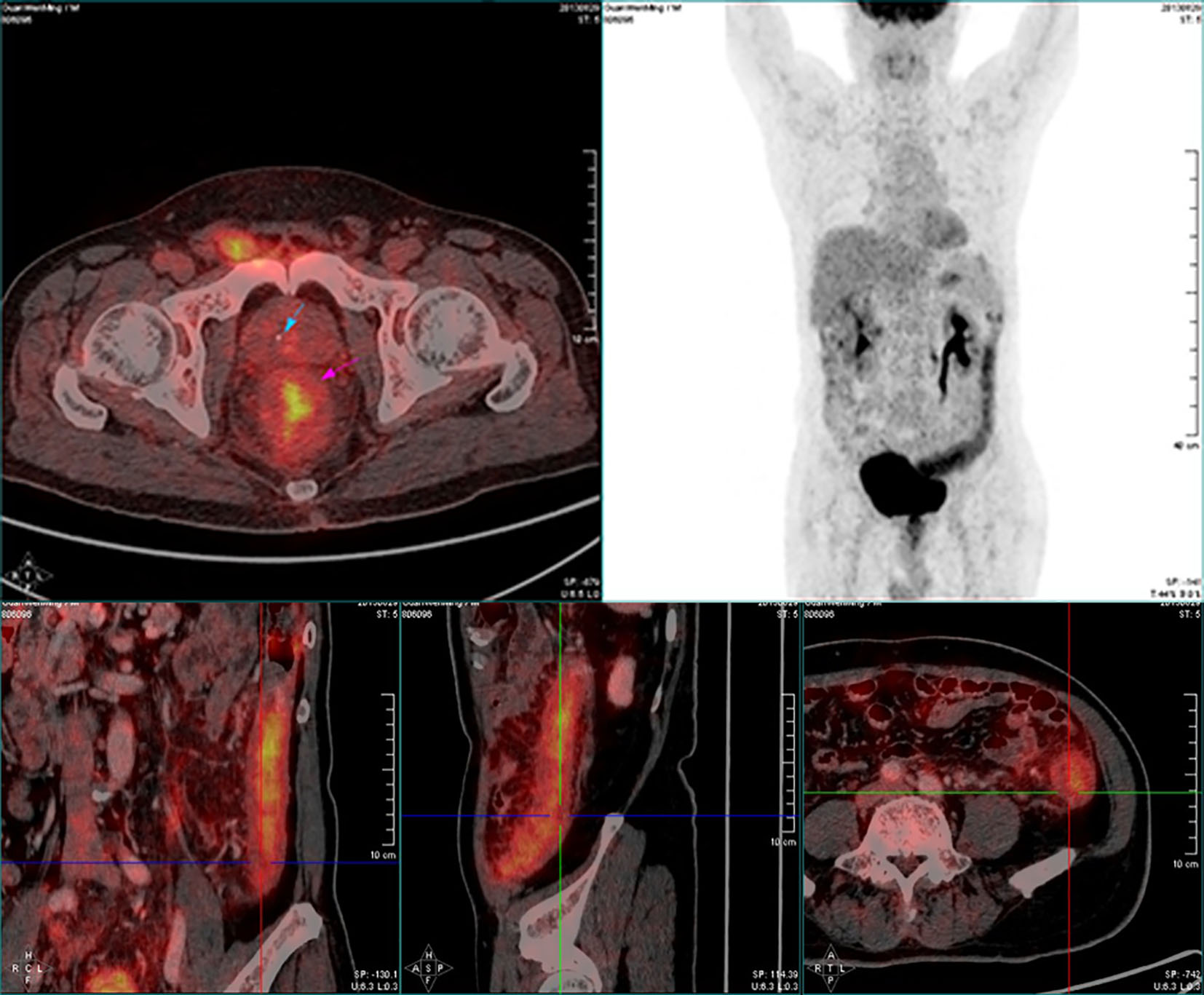
Figure 6. PET-CT of the abdomen showed significant accumulation of FDG uptake (SUV max: 5.7), diffuse edema and thickening (about 1.5 cm) of the distal descending colon wall, indicating an inflammatory lesion.
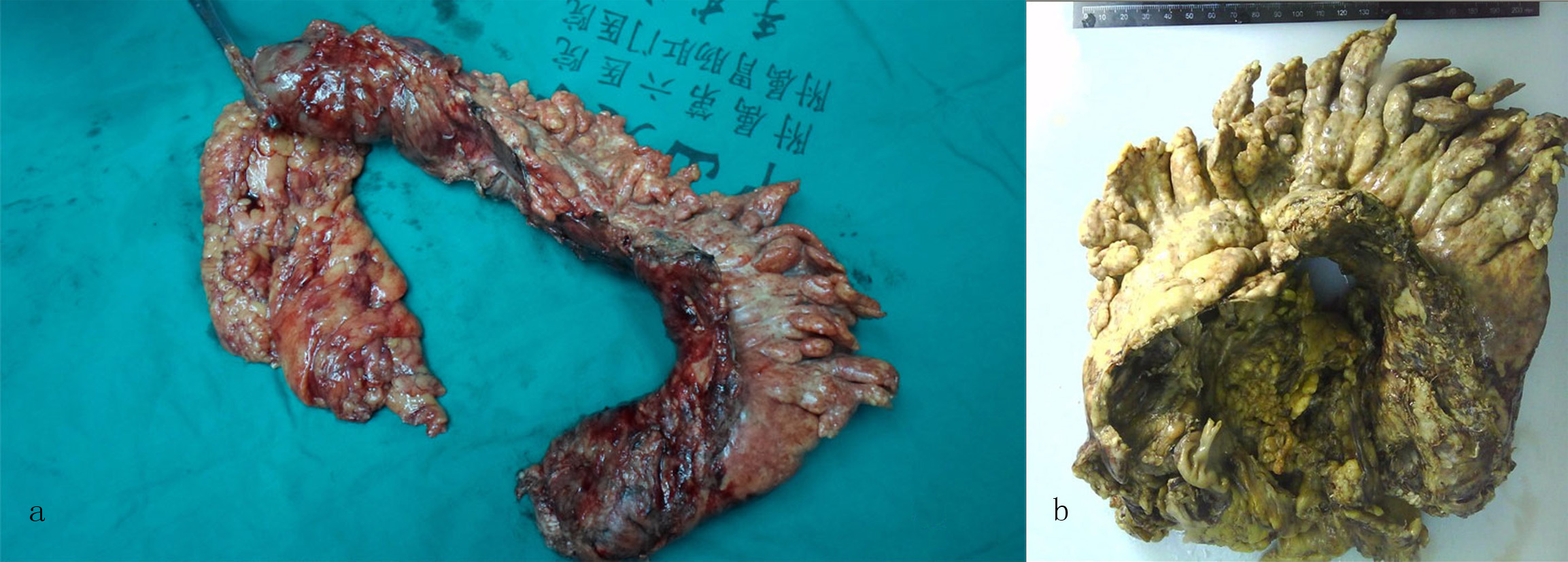
Figure 7. Macroscopic examination of the partial colectomy revealed (a) a 48 cm segment of stiff bowel and (b) a 48 × 7 × 6 cm portion of stiff mesentery.
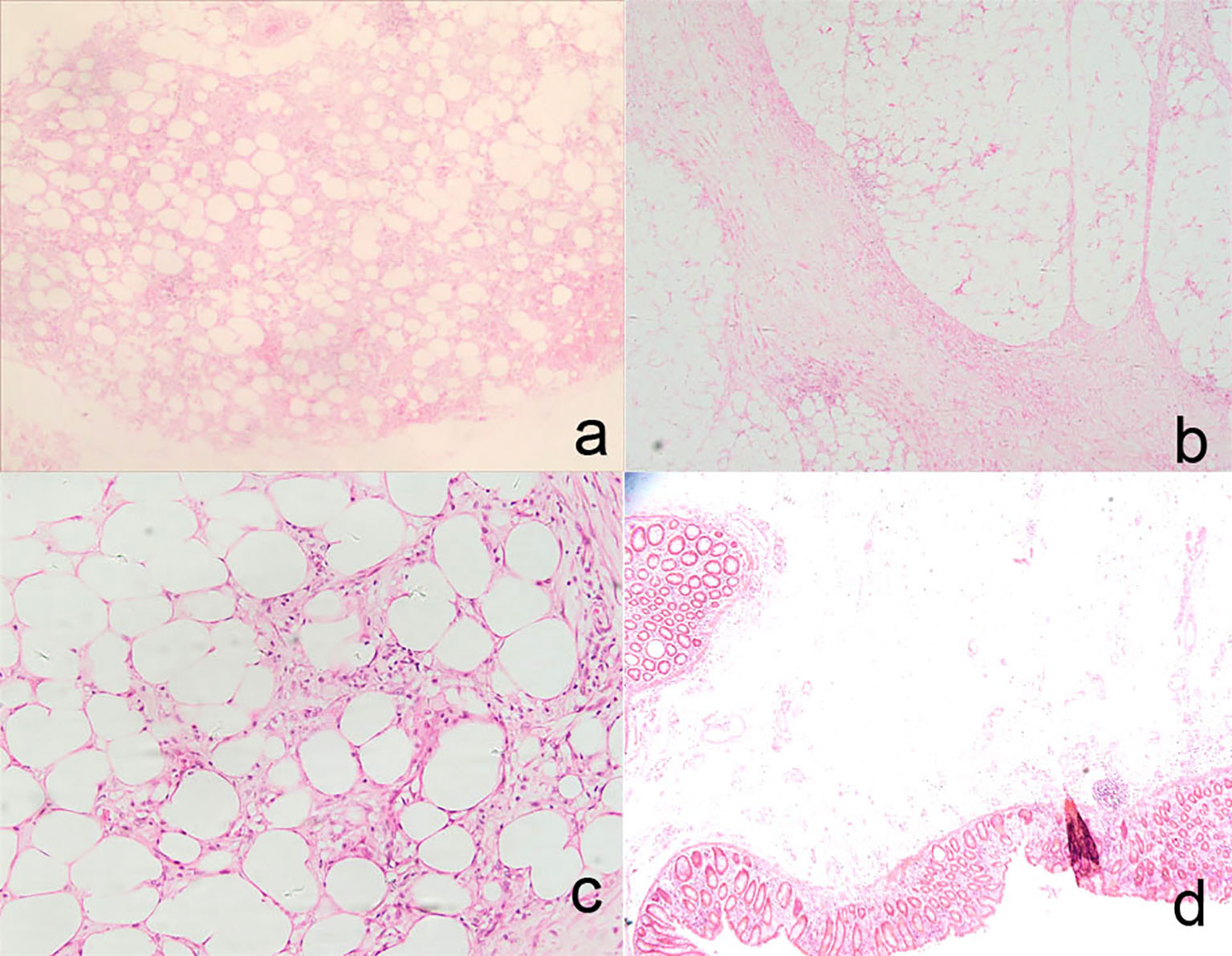
Figure 8. Histologic findings in the partial colectomy and mesentery included fat necrosis and multifocality lipid-filled macrophages in mesentery adipose tissue (H&E staining, × 4, a), multifocality fibrosis in mesentery adipose tissue (H&E staining, × 4, b; H&E staining, × 20, c), markedly edematous submucosa and partially eroded and hemorrhagic mucosa (H&E staining, × 2.5, d).
Table
Table 1. Radiographic Features of Sclerosing Mesenteritis
| Thickness of the involved mesentery |
| Increased fat density |
| Fibrosis and enlarged lymph nodes |
| Fat ring sign |
| Pseudocapsule |
| Dilated or engorged mesenteric vessels |
| Well-defined or poorly defined mesenteric mass |
| Strand-like densities around the mesenteric vessels |
| Well-defined soft tissue nodules (usually less than 5 mm) |
| Bowel obstruction |