Figures
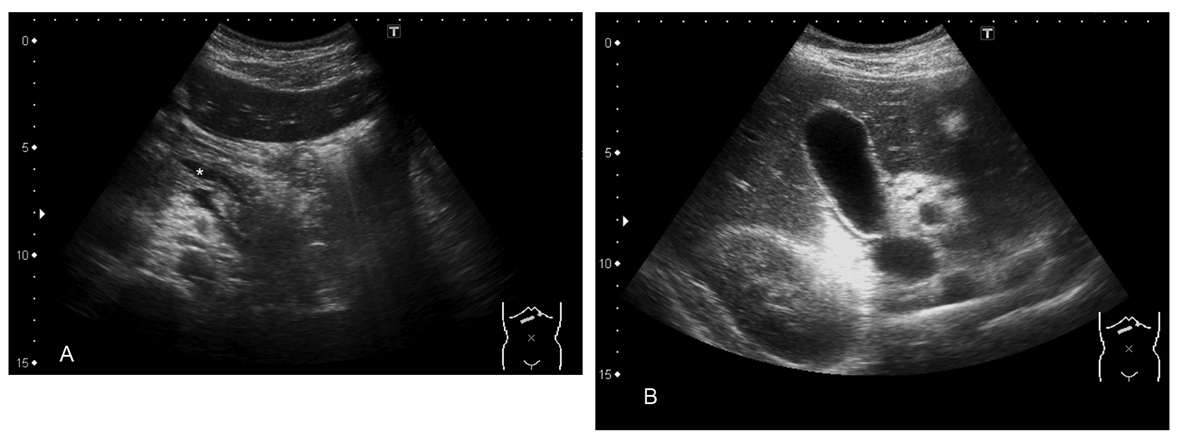
Figure 1. A) Pancreas and dilated duct (asterisk); B). Normal gallbladder.
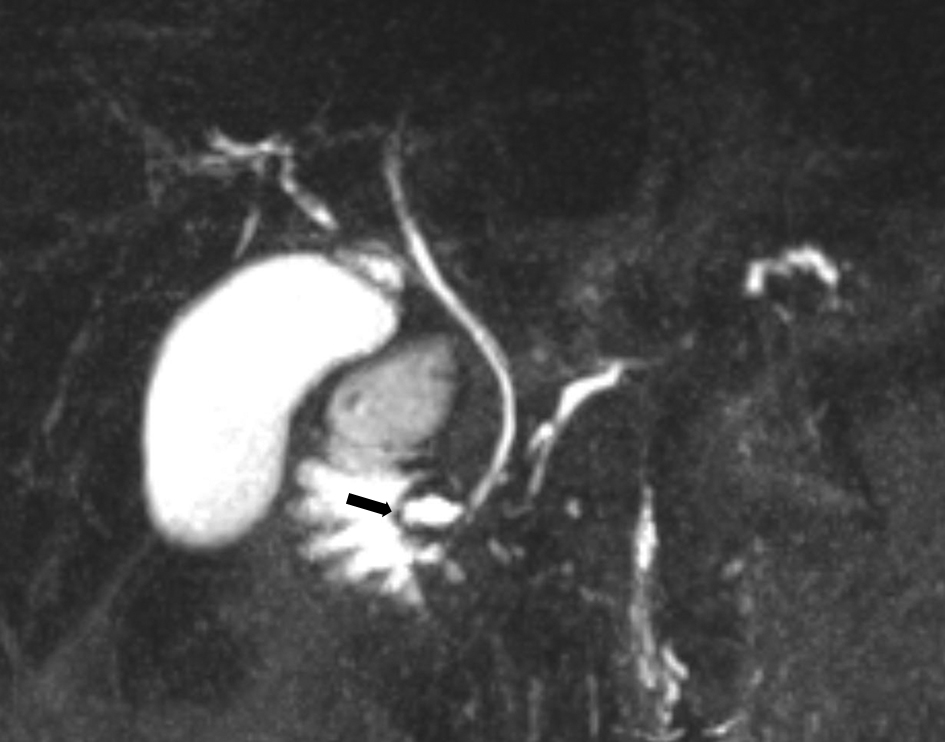
Figure 2. Pre-endoscopic treatment; 40 mm coronal MIP reformat of MRCP. The common bile duct runs to the major papilla. The pancreatic duct drains through the minor papilla (arrow).
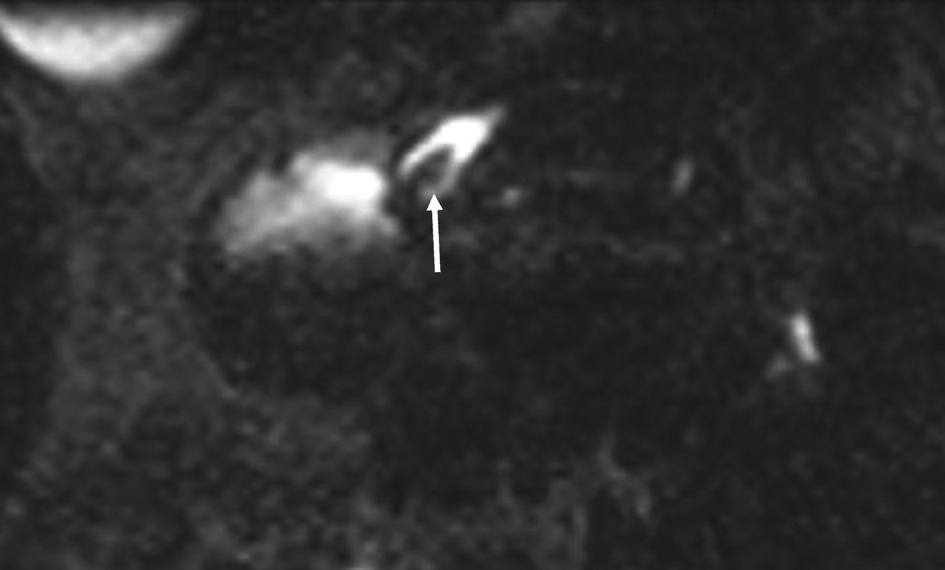
Figure 3. Pre endoscopic treatment; 3 mm axial MPR reformat through the minor papilla. The stone (arrow) is clearly visible in the ampulla of the accessory pancreatic duct.
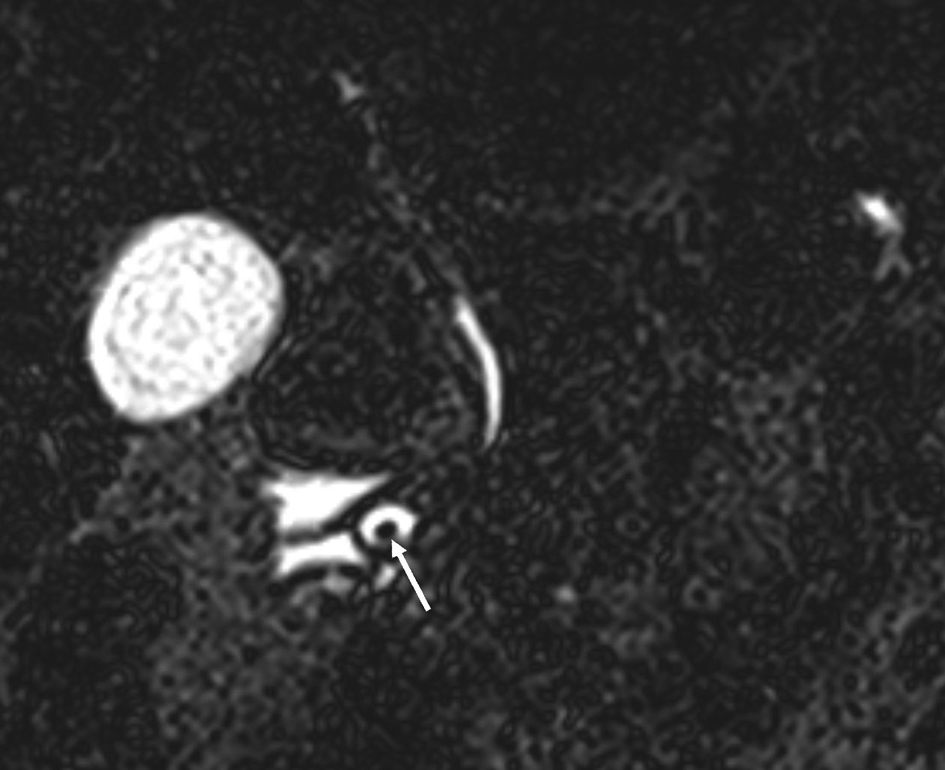
Figure 4. Original pre-treatment; 1 mm coronal MRCP-slice at the level of the minor papilla. The stone (arrow) in the ampulla on the accessory pancreatic duct is clearly visible.
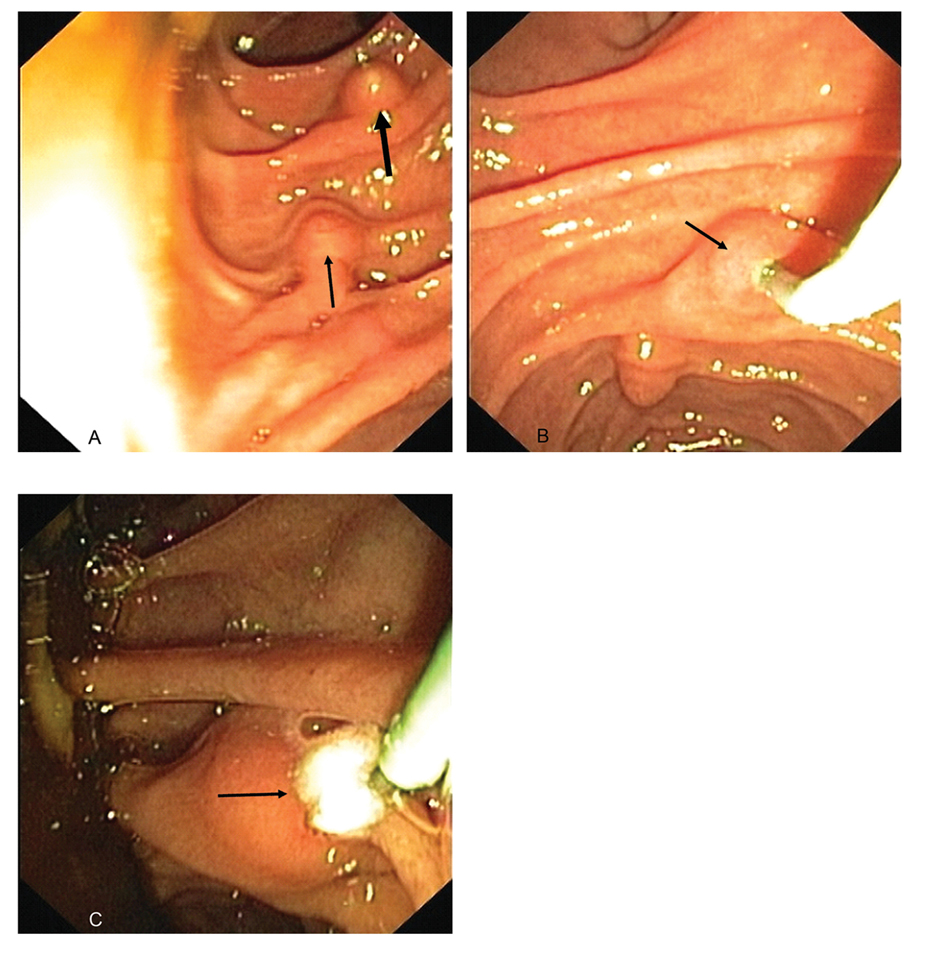
Figure 5. A). An endoscopic view from the papilla major (thick arrow) and more distal papilla minor (thin arrow); B). The minor papilla (arrow) was cannulated; C). The stone (arrow) was removed into the duodenum.
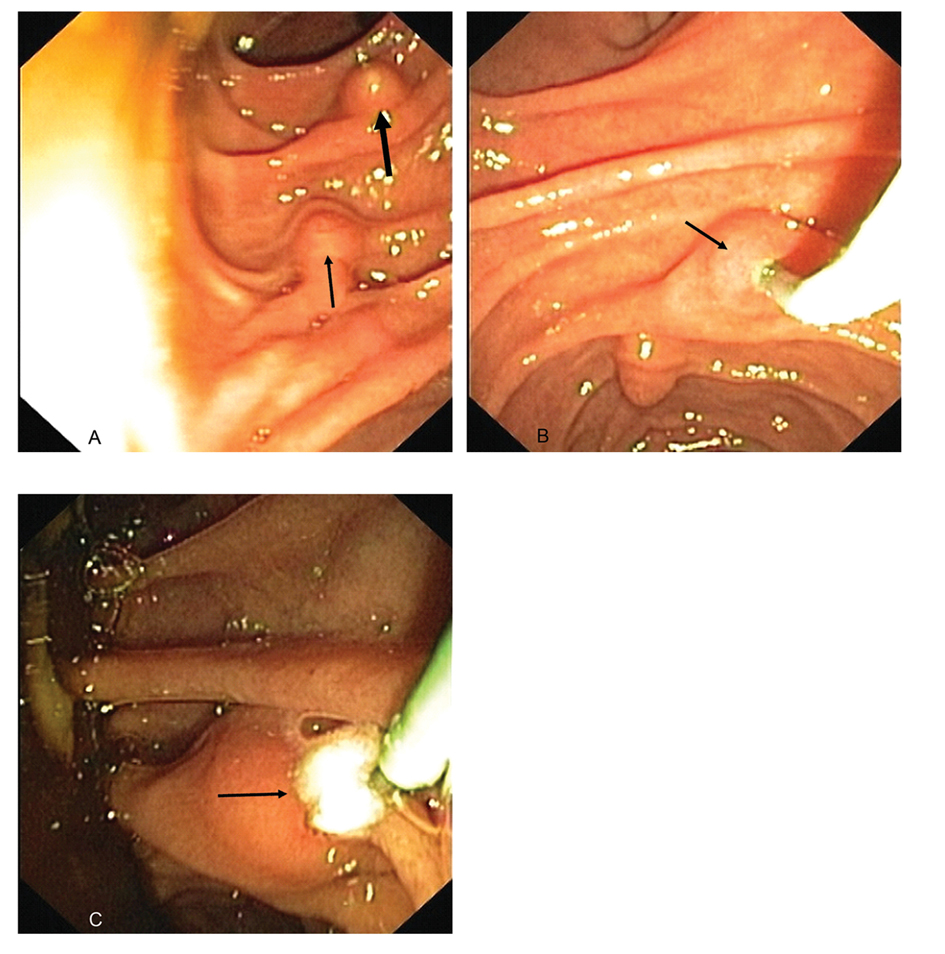
Figure 6. Post endoscopic treatment; 40 mm coronal MIP reformat of the MRCP. The ampulla of the accessory pancreatic duct is no longer visible.