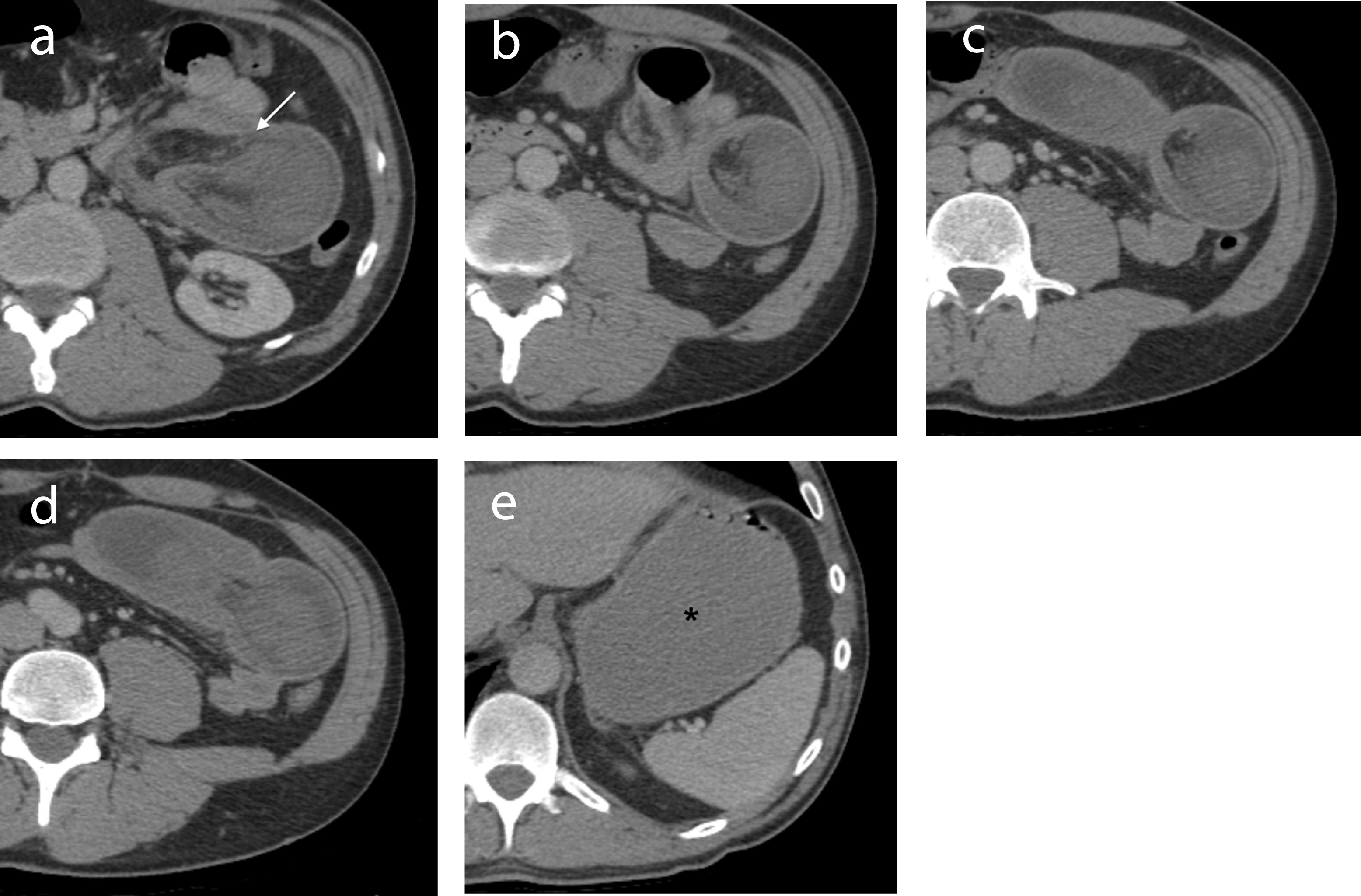
Figure 1. (a-d) IV contrast-enhanced axial CT images through the abdomen demonstrate a jejunal intussusception on the left side with proximal obstruction. The dilated intussuscepiens contains the intussusceptum along with mesenteric fat and vessels (arrow). (e) The stomach is distended (*). The 2.5 cm GIST causing the intussusception is not seen on CT.

Figure 2. (a) The gross specimen consisted of an intussuscepted segment of small bowel. (b) A 2.5 cm solitary, well-circumscribed neoplasm with hemorrhagic cut surfaces was present at the base of the intussusception arising from within the submucosa and muscularis propria. The serosa was intact and the mesentery was uninvolved.
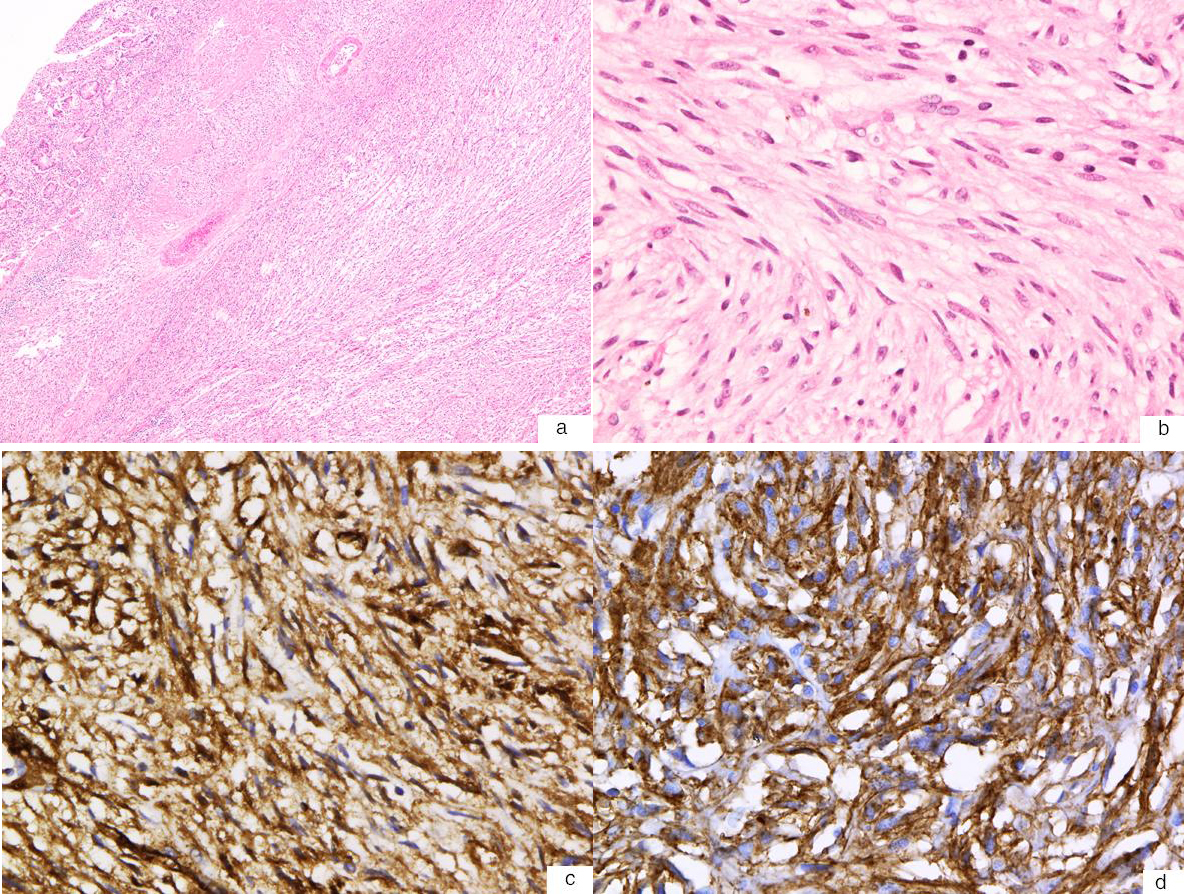
Figure 3. (a) Hematoxylin and eosin stain of the GIST shows a spindle cell neoplasm with a relatively low cellular density (40X). (b) High-power magnification (400X) shows that the neoplasm is comprised of interlacing bundles of bland spindle cells with fibrillary eosinophilic cytoplasm with a paucity of mitotic figures (0 mitosis per high-power field). (c) Immunohistochemistry stain shows that the tumour cells are immunoreactive for CD34 (400X). (d) Immunohistochemistry stain also shows that the tumour cells are immunoreactive for c-kit (CD117) (400X).