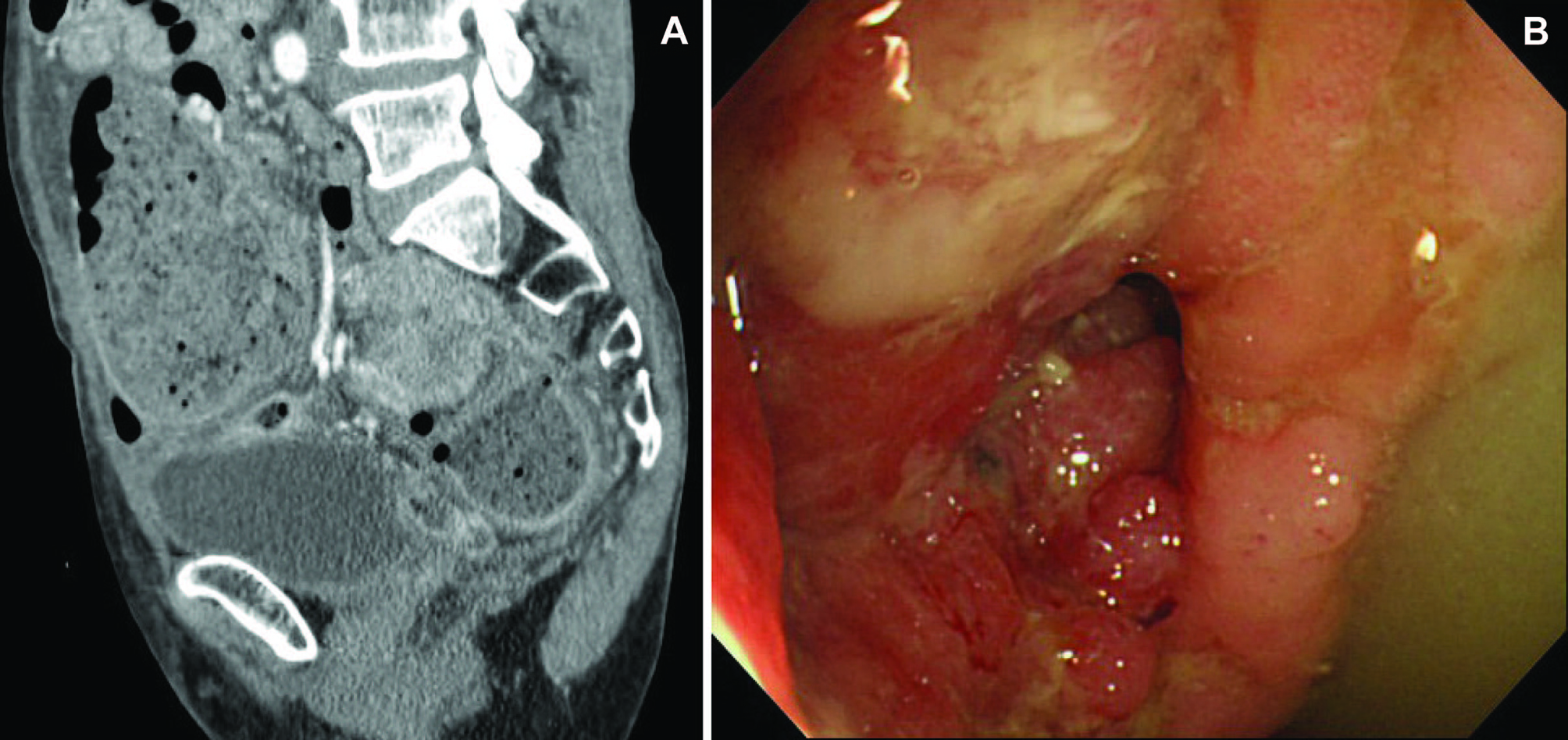
Figure 1. (A) Abdominal CT showing sigmoid carcinoma and the dilated colon; (B) Sigmoid carcinoma showing the obstructed lumen which can be detected.
| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Original Article
Volume 3, Number 5, October 2010, pages 201-206
Techniques and Outcomes of Endoscopic Decompression Using Transanal Drainage Tube Placement for Acute Left-sided Colorectal Obstruction
Figures
Tables
| No. (%) | |
|---|---|
| *Except for age, the number of the patient is shown. | |
| Age (mean ± SD)* | 71 ± 12 |
| Gender (M/F) | 36/33 (52/48) |
| Etiology: | |
| Colorectal carcinoma | 66 (96) |
| Pancreas carcinoma | 1 (1) |
| Postoperative stenosis | 1 (1) |
| Intussusception | 1 (1) |
| Obstruction location: | |
| Sigmoid colon | 37 (54) |
| Rectum | 20 (29) |
| Descending colon | 12 (17) |
| Major symptoms: | |
| Abdominal pain | 69 (100) |
| Constipation | 69 (100) |
| Bloating | 69 (100) |
| Nausea/vomiting | 60 (87) |
| Obstruction Location | Patient Number | Successful Procedure | Procedure Time (min) | Method A GW+TDT | Method B GC+BGW+TDT | Method C GC+BGW+DL+TDT |
|---|---|---|---|---|---|---|
| Procedure time (min) is shown as mean ± SD. | ||||||
| GW, guidewire; TDT, transanal drainage tube; GC, guide catheter; BGW, biliary guidewire; DL, dilator. | ||||||
| *A small-diameter upper endoscope was used. | ||||||
| Rectum | 20 | 20 (100%) | 15 ± 6 | 16 | 4 | 0 |
| Sigmoid colon | 35 | 32 (91%) | 33 ± 12 | 18 | 14 | 3 |
| Descending colon | 12 | 12 (100%) | 27 ± 12 | 9 | 1 | 2 |
| Sigmoid | 2 | 2 (100%) | 25 | 2* | 0 | 0 |
| 69 | 66 (96%) | 27 ± 13 | 45 (65%) | 19 (28%) | 5 (7%) | |