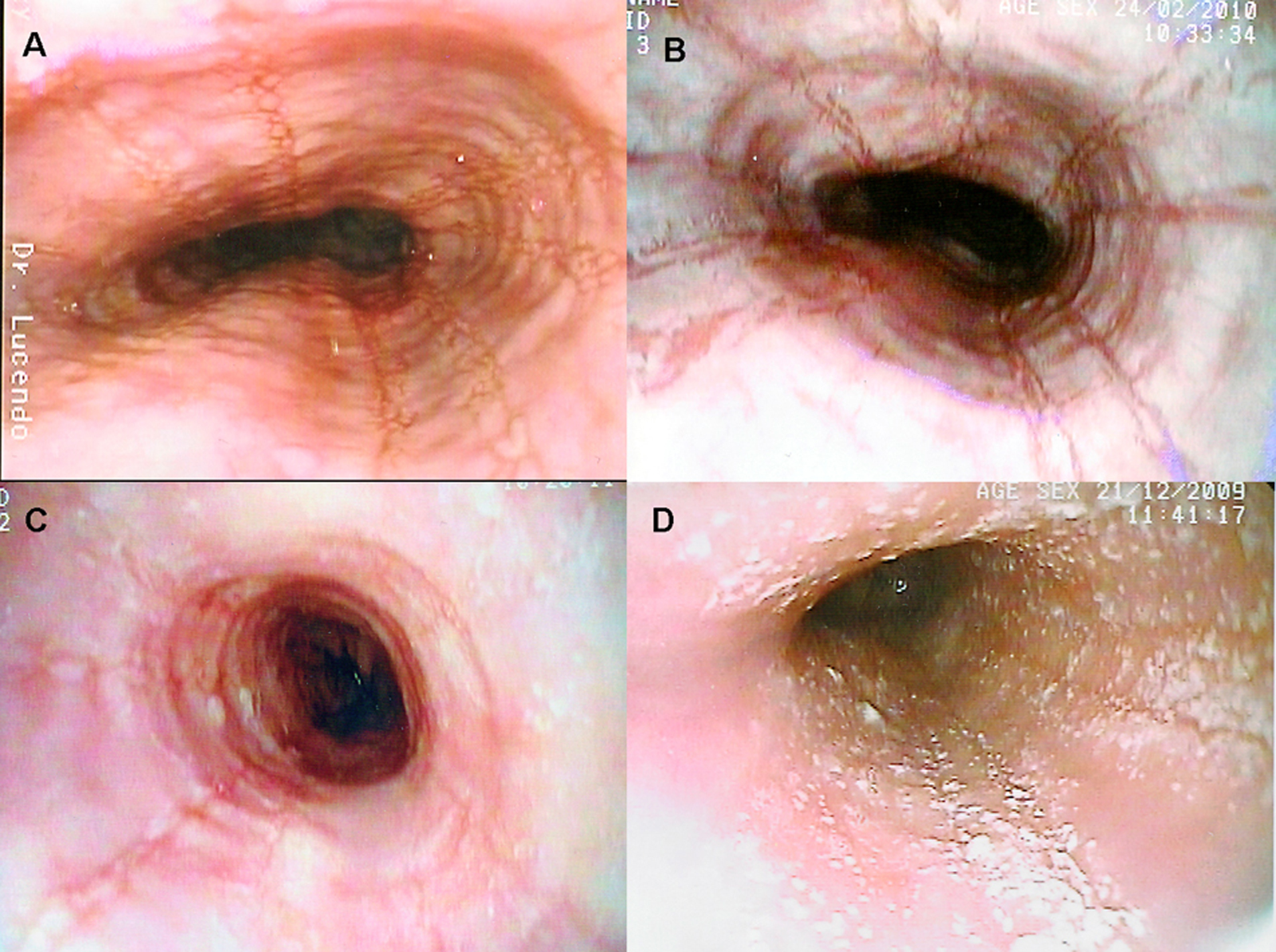
Figure 1. Several endoscopic aspects of eosinophilic esophagitis. A: Normal-caliber esophagus with longitudinal linear furrows and irregular mucosa. B: Fragile-looking mucosa, which comes loose with biopsy forceps, and marked mucosal corrugation. C: Reduced-caliber, trachealized esophagus with irregular, cobblestone appearance. D: The esophageal mucosal surface may be covered in cotton-like exudates mimicking candiadiasis, but biopsy finds them to be multiple eosinophil-containing micro-abscesses.
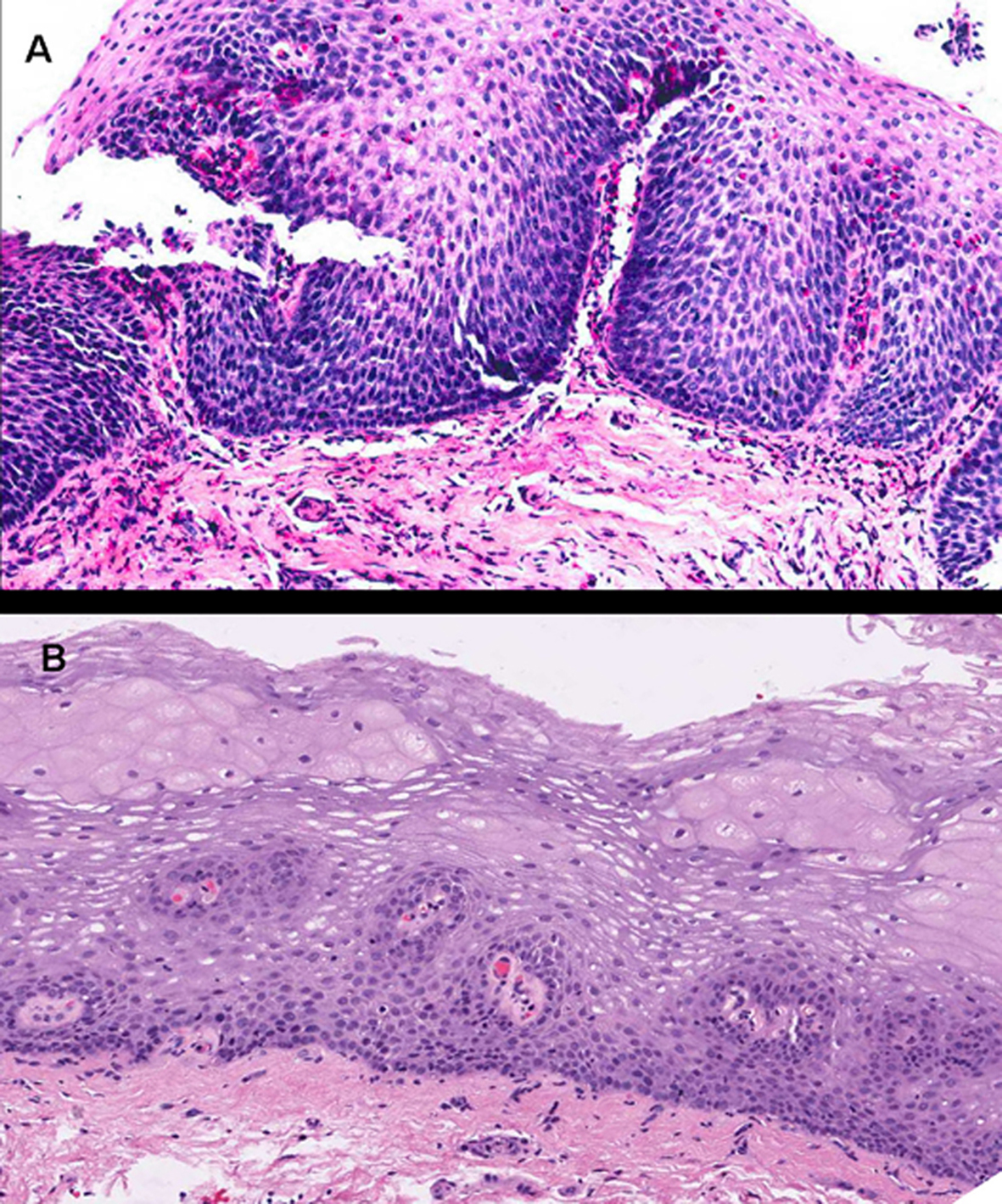
Figure 2. Images corresponding to the same patient before and after therapy with topical fluticasone propionate to illustrate changes in the esophageal epithelium. A: Marked epithelial proliferation with basal-cell hyperplasia reaching up to superficial strata, in addition to elongated connective papillas, which appear thicker and hypervascularized. Numerous eosinophils infiltrate into the epithelium. B: Obtained after 3 months under treatment with fluticasone propionate. The esophageal epithelium exhibits fewer cells and recovered stratification, with basal cells occupying not more than 15% of esophageal thickness, and no eosinophilic infiltration (hematoxylin and eosin, x200).