Figures
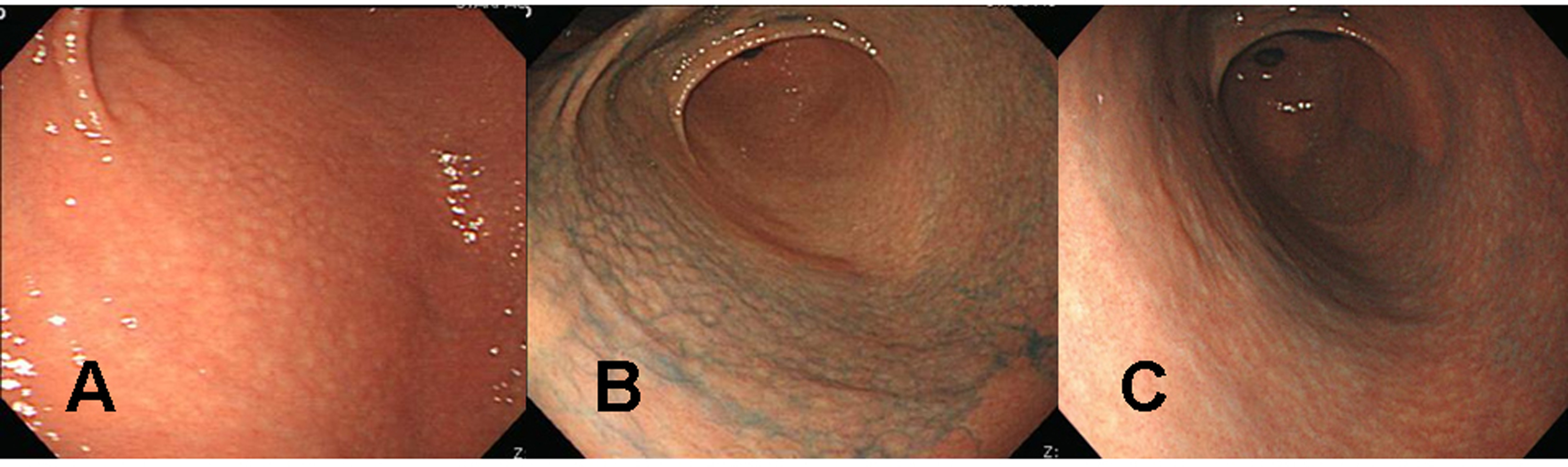
Figure 1. Endoscopic findings of the proximal antrum in the first patient (a 39 years old woman). (A) Initial findings showed micronodules measuring 2-5 mm in diameter with a smooth surface. The findings are observed from the antrum to the low corpus of the stomach, indicating a diffuse-type nodular gastritis. (B) There were no remarkable changes in nodular elevation on chromoendoscopic findings 1 month after H. pylori eradication, even after applying 0.2% indigo carmine spray. There was also no change in diffuse-type nodular gastritis since the previous examination. (C) Indigo carmine (0.2%) chromoendoscopy conducted 3 months after successful H. pylori eradication revealed, diminished nodular elevations.
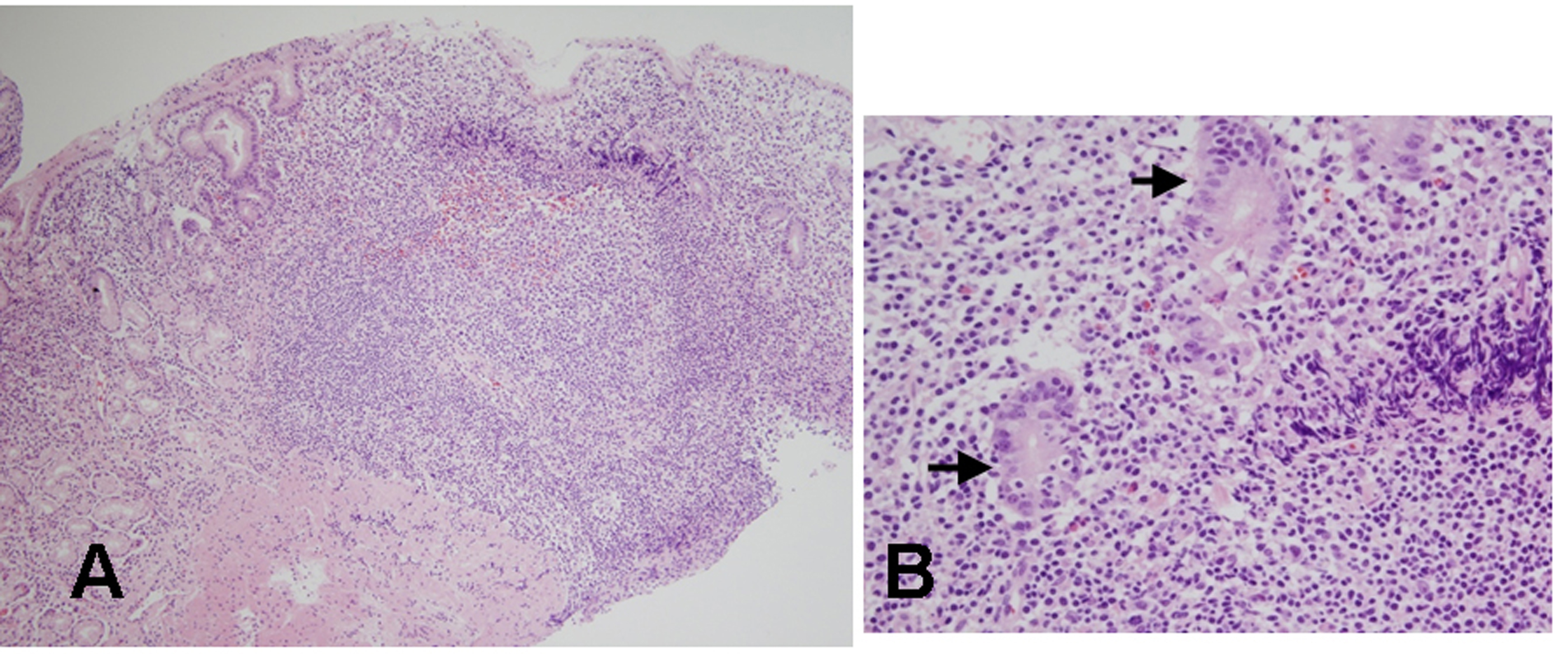
Figure 2. Histologic findings of biopsied specimens from the anterior aspect of the antrum in the first patient. (A) On microscopic findings at a low magnification, the nodular mucosa is expanded by a marked lymphoplasma cell infiltration with the presence of a prominent germinal center (H&E stain, x100). (B) On microscopic findings at a higher magnification, diffuse lymphoplasma cell infiltration is noted in the lamina propria, and a few lymphocytes are infiltrating the epithelium. Low grade gastric MALT lymphoma is suspected, but no definite lymphoepithelial lesion is found (H&E stain, x400).
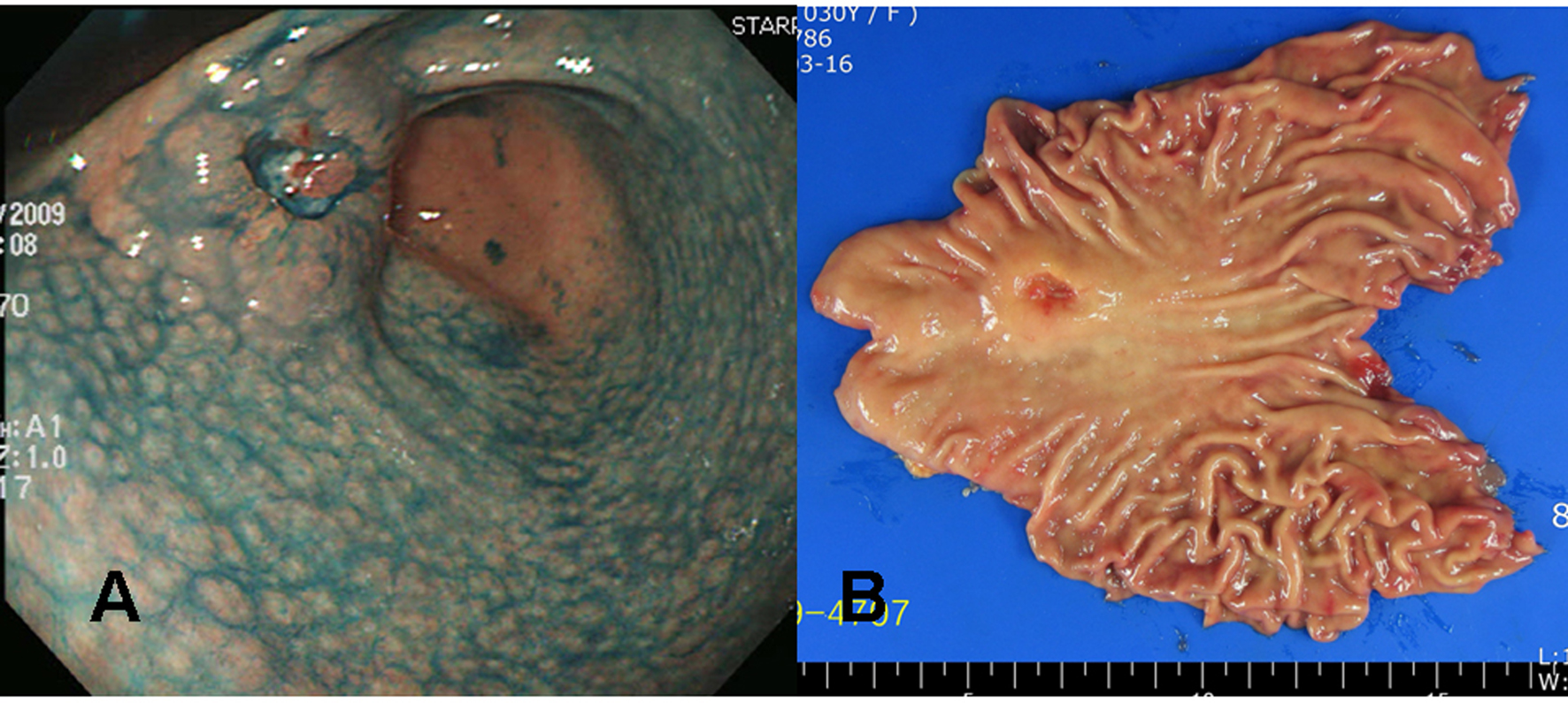
Figure 3. Gross findings of endoscopy and surgical specimens in the second patient (a 30 years old woman). (A) Chromoendoscopic findings with application of 0.2% indigo carmine showed diffuse mucosal nodularity evident on the antrum and lower corpus of the stomach, leading to a diagnosis of diffuse-type nodular gastritis. A round, elevated lesion with central ulceration can be seen on the anterior aspect of the proximal antrum. The edge and base of the ulcer are irregular and uneven, suggesting a cancerous change. (B) A 3.2 x 2.0 x 1.0 cm Borrmann type III gastric cancer was completely resected surgically by subtotal gastrectomy, with negative resection margins.
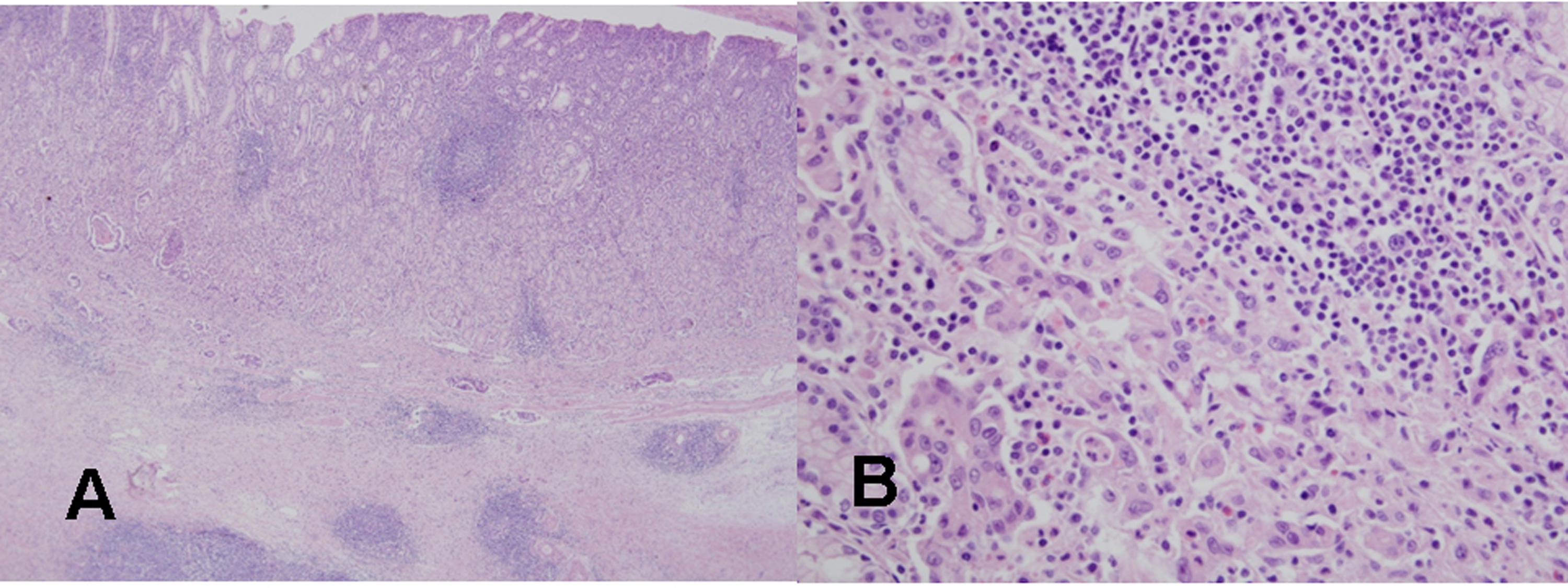
Figure 4. Histological findings of the resected gastric cancer in the second patient. (A) On microscopic findings at a low magnification, mononuclear cell infiltration with germinal centers is noted in the mucosa and submucosa around the gastric cancer (H&E stain, x40). (B) On microscopic findings at a higher magnification, a poorly differentiated tubular adenocarcinoma is evident near the lymphoid follicle in the mucosa (H&E stain, x400).
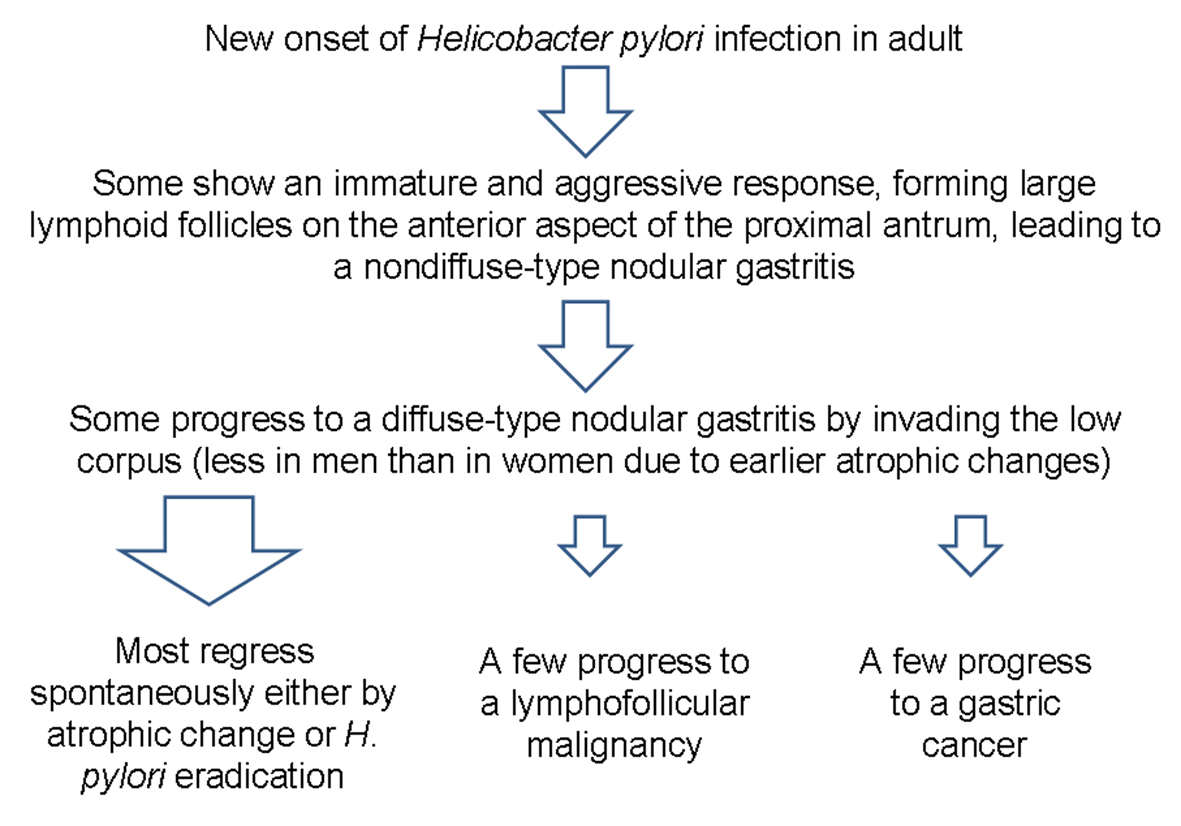
Figure 5. Schema of the progression of nodular gastritis to gastric neoplasms. In contrast to the case in children, novel H. pylori infection may lead to nodular gastritis in some adults, and some may progress to a diffuse-type nodular gastritis that invades both the antrum and body. A few cases of diffuse-type nodular gastritis may progress further to gastric neoplasm, especially in young women, due to fewer atrophic changes.