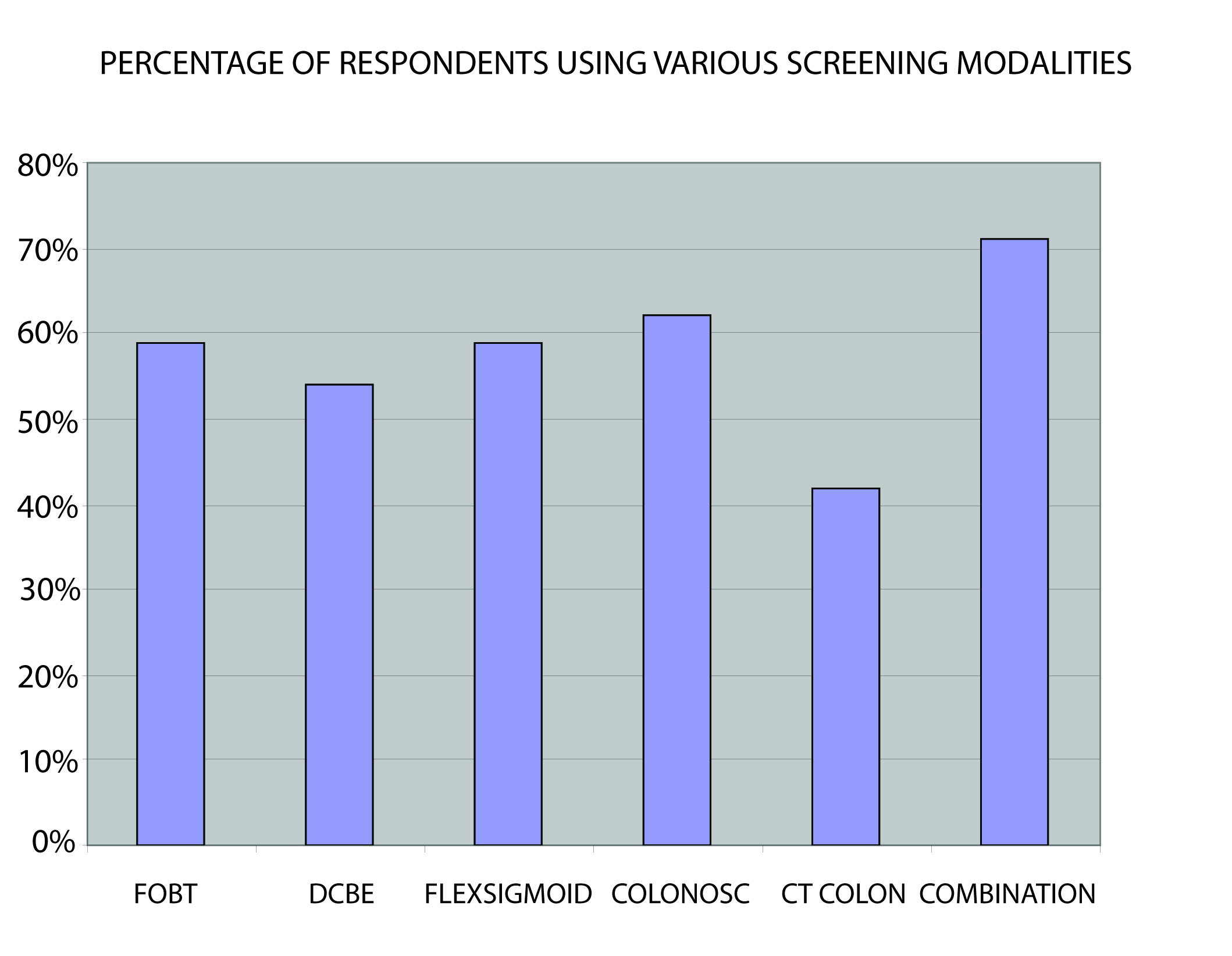
Figure 1. The screening methods. FOBT, Faecal occult blood test; DCBE, Double contrast barium enema; FLEX SIGMOID, Flexible Sigmoidoscopy; COLONOSC, Colonoscopy; CT COLON, CT Colonography; COMBINATION, Combination of 2 screening methods (Faecal occult blood test with double contrast barium enema or Sigmoidoscopy).