Figures
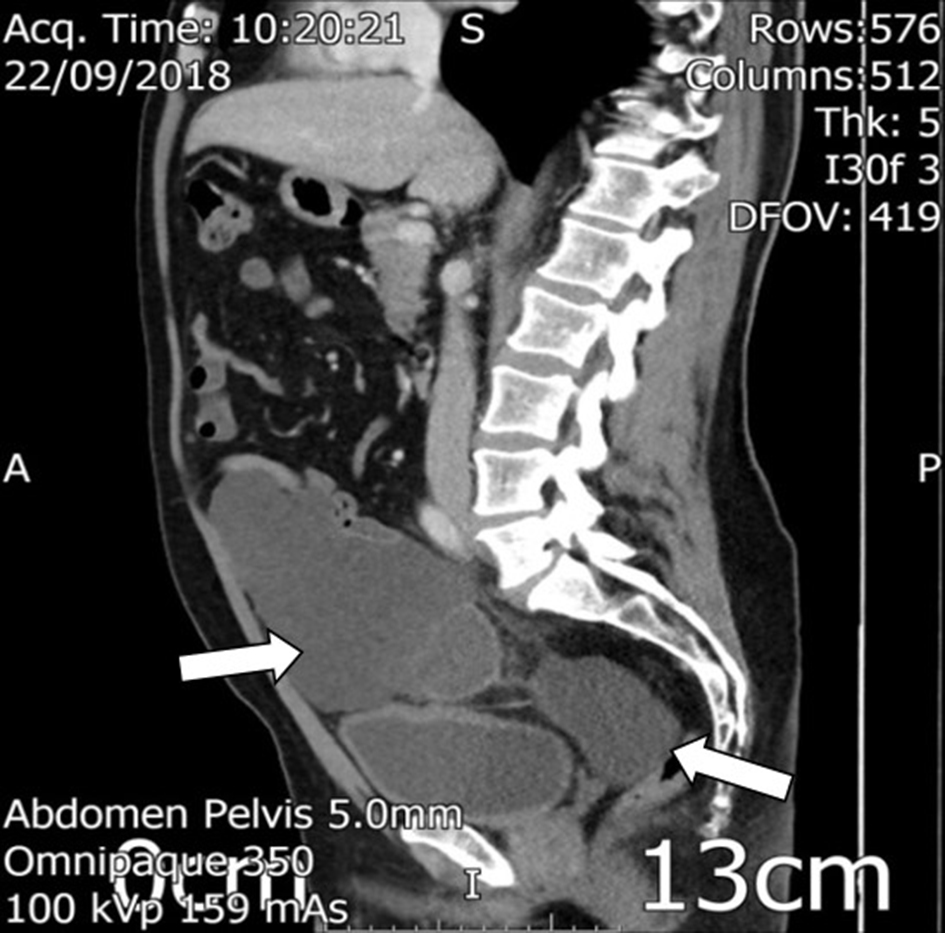
Figure 1. Sagittal view of the right iliac fossa mass and pelvic deposits in the cul-du-sac.

Figure 2. Coronal view of the right iliac fossa mass, demonstarting an enhancing, irregular wall at its inferior aspect, being suggestive of likely appendiceal abscess.
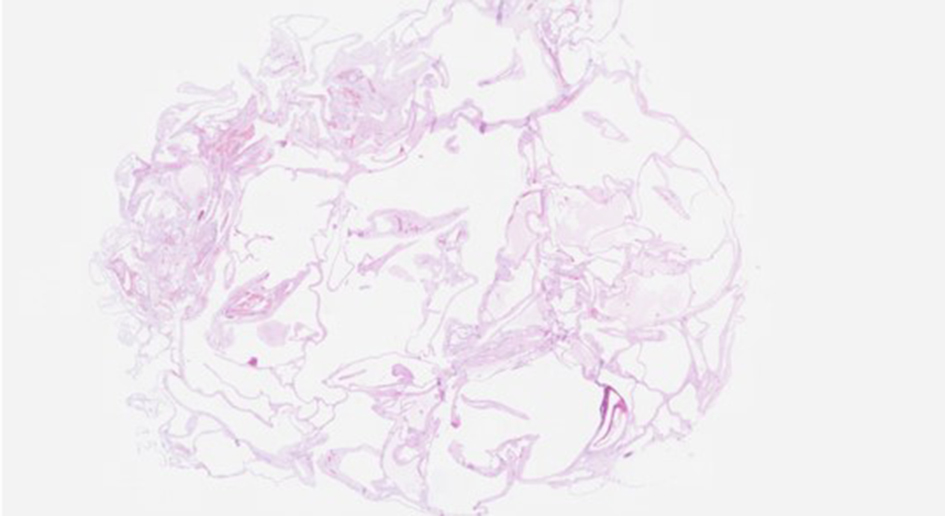
Figure 3. H&E × 5 magnification: section from the nodular lesion on the serosal aspect of terminal ileum. Low magnification view showing a serosal lesion with multiple cystic spaces of varying sizes. H&E: hematoxylin and eosin.
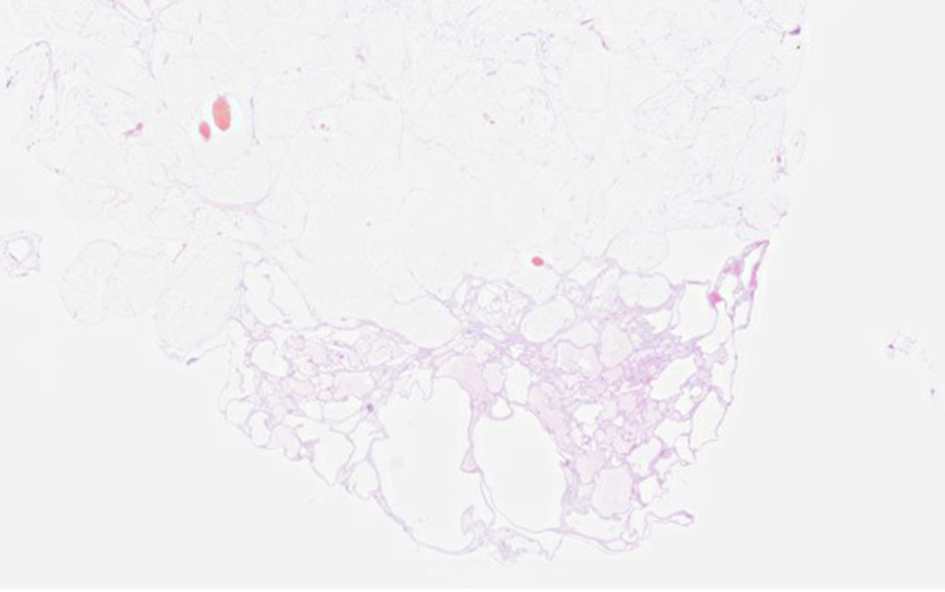
Figure 4. H&E × 5 magnification: representative section from the multicystic lesion present on the serosal aspect of the cecum. H&E: hematoxylin and eosin.
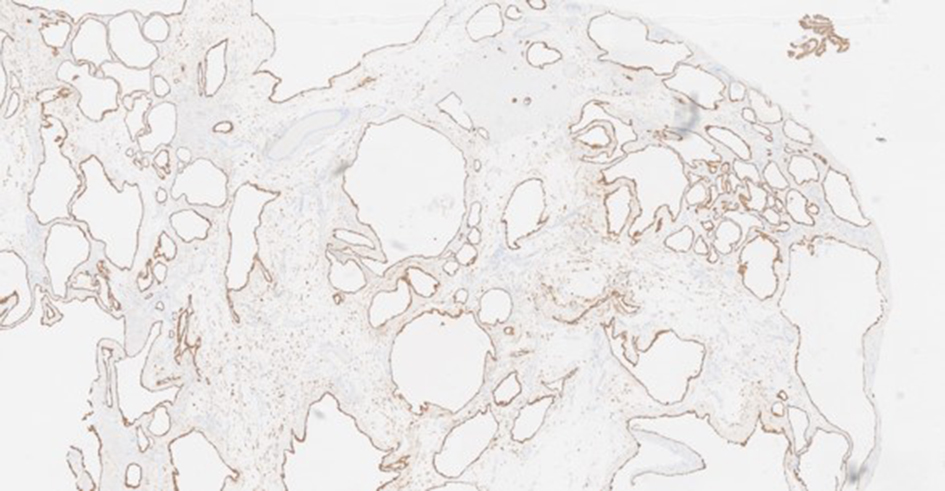
Figure 5. MNF × 20 magnification: cytokeratin MNF116 immunostain highlights the lining cells which are positive.
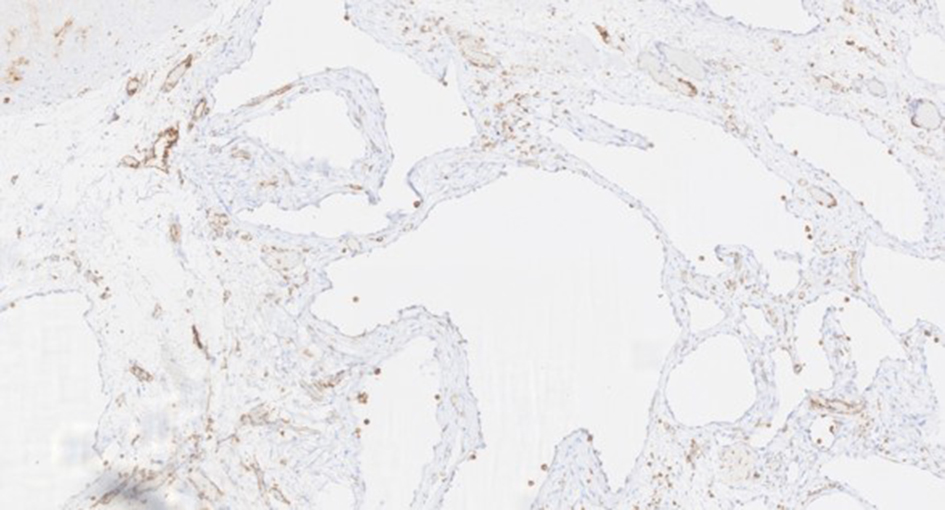
Figure 6. CD31 × 100 magnification: the lining cells are negative for CD31 immunostain indicating that these are not endothelial cells thereby excluding a lymphangioma or a hemangioma. The blood vessels in between the cystic spaces are highlighted.
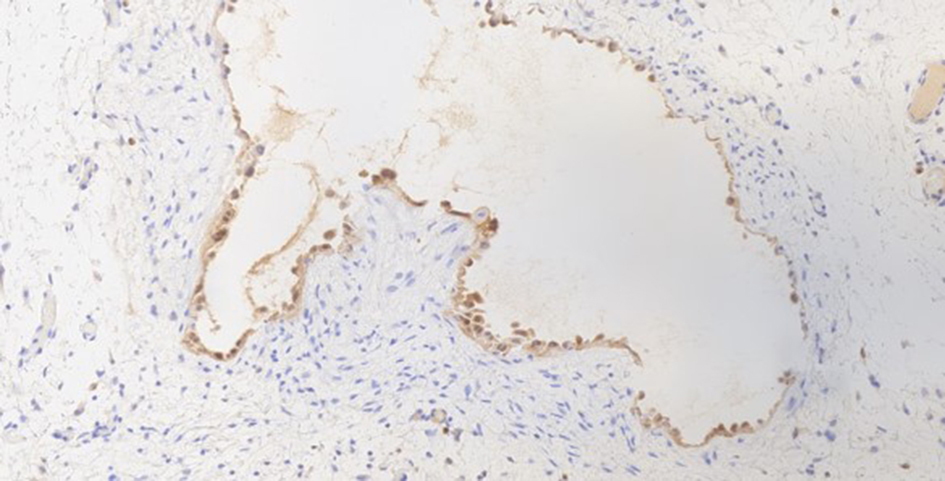
Figure 7. Calretinin × 200 magnification: the lining cells are positive for calretinin immunostain in keeping with mesothelial origin.