Figures
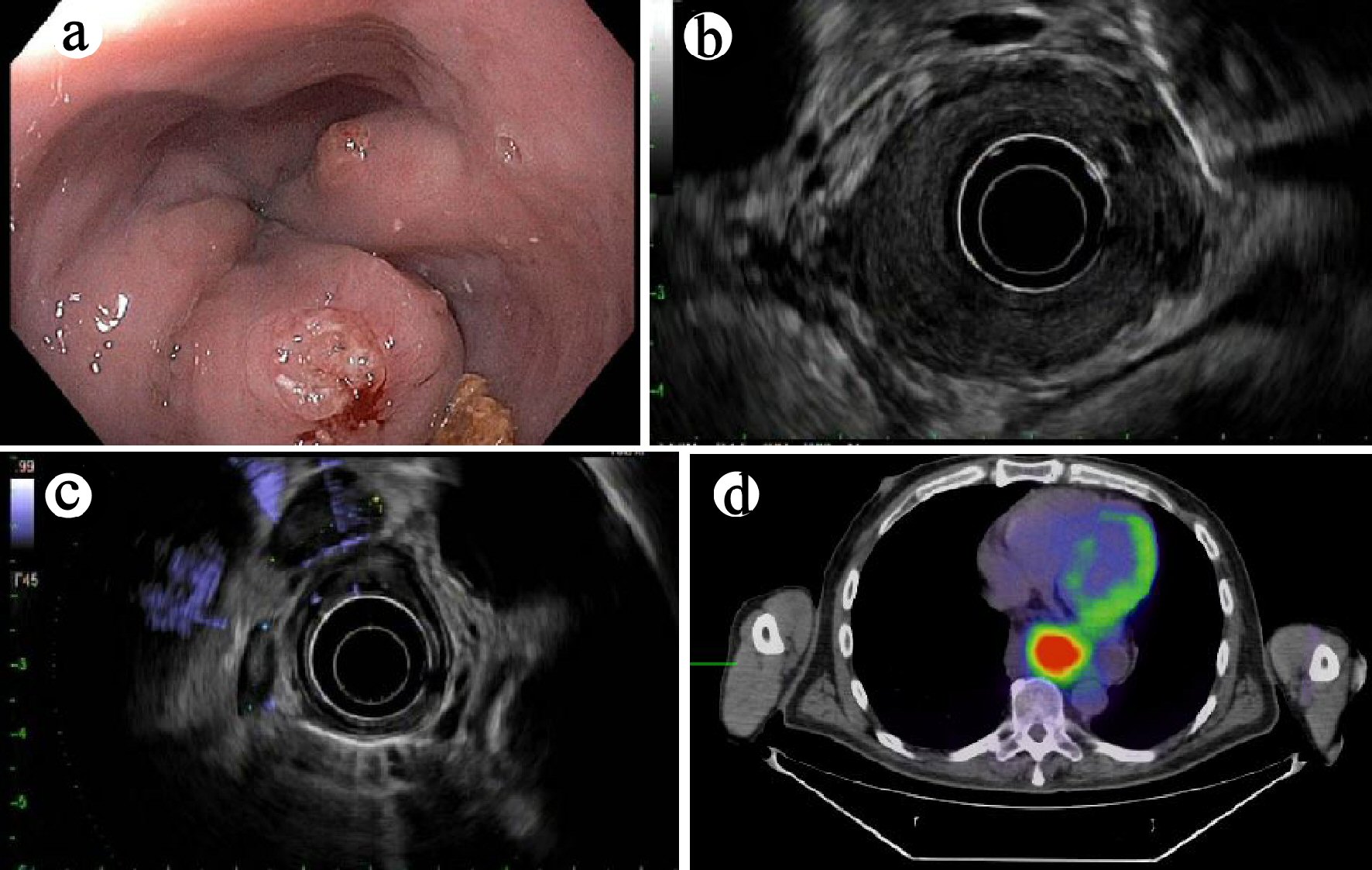
Figure 1. (a) Endoscopic finding of an esophageal mass on esophagogastroduodenoscopy (case 1). (b) Mural destruction by the mass on endoscopic ultrasound (EUS) examination. (c) Enlarged hypoechoic nodes, suspicious for metastases on EUS examination. (d) Positron emission tomography (PET) revealed a hypermetabolic mass in the distal esophagus (axial view).
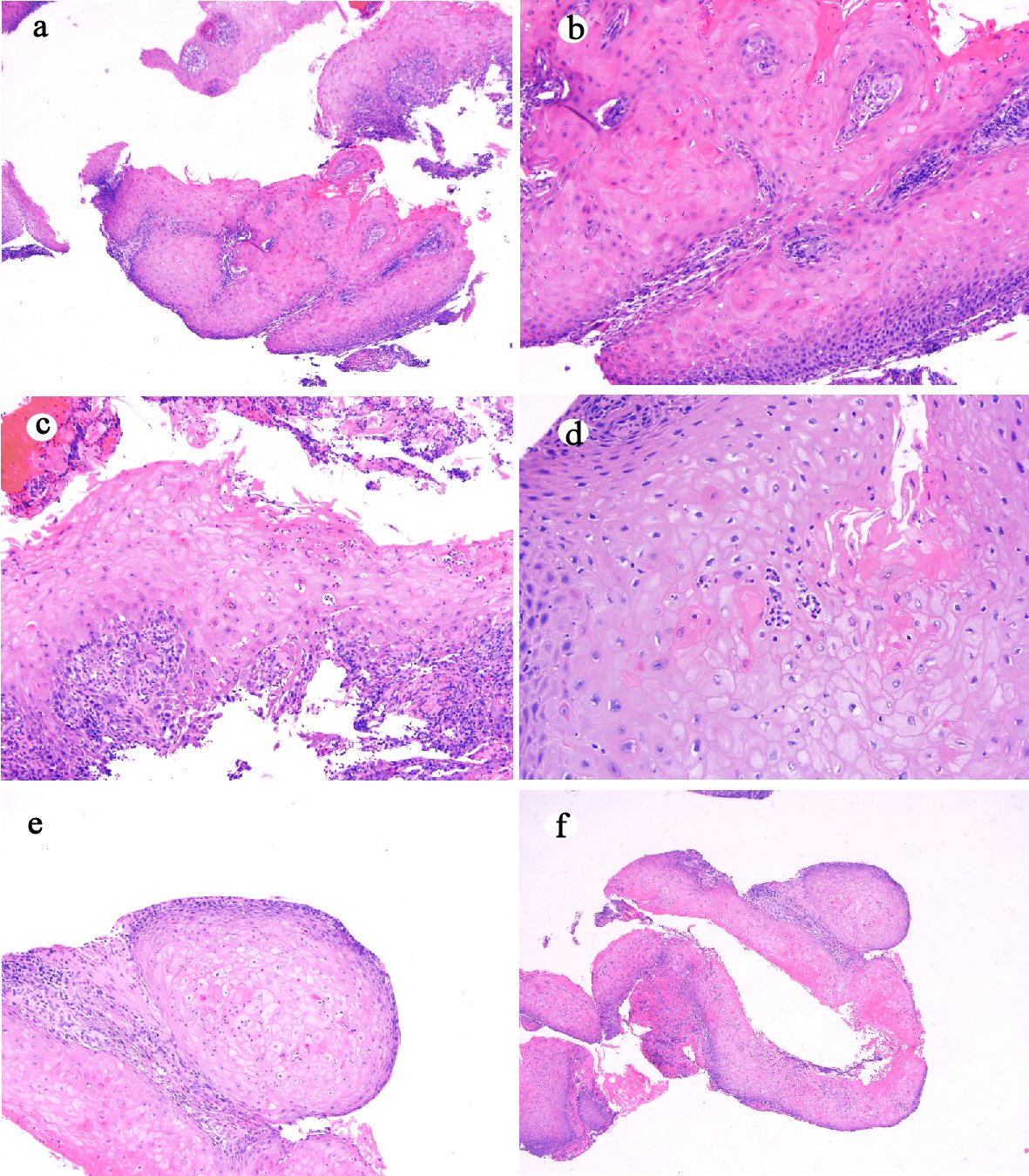
Figure 2. Histologic features of mucosal biopsy from the mass (case 1). Squamous epithelium shows hyperkeratosis and acanthosis ((a) hematoxylin and eosin stain, original magnification × 40), focal atypia ((b) hematoxylin and eosin stain, original magnification × 200), intraepithelial neutrophilic inflammation and microabscesses and dyskeratosis ((c) hematoxylin and eosin stain, original magnification × 200), koilocyte-like cells ((d) hematoxylin and eosin stain, original magnification × 200), deep keratinization ((e) hematoxylin and eosin stain, original magnification × 100), and furrow ((f) hematoxylin and eosin stain, original magnification × 20).
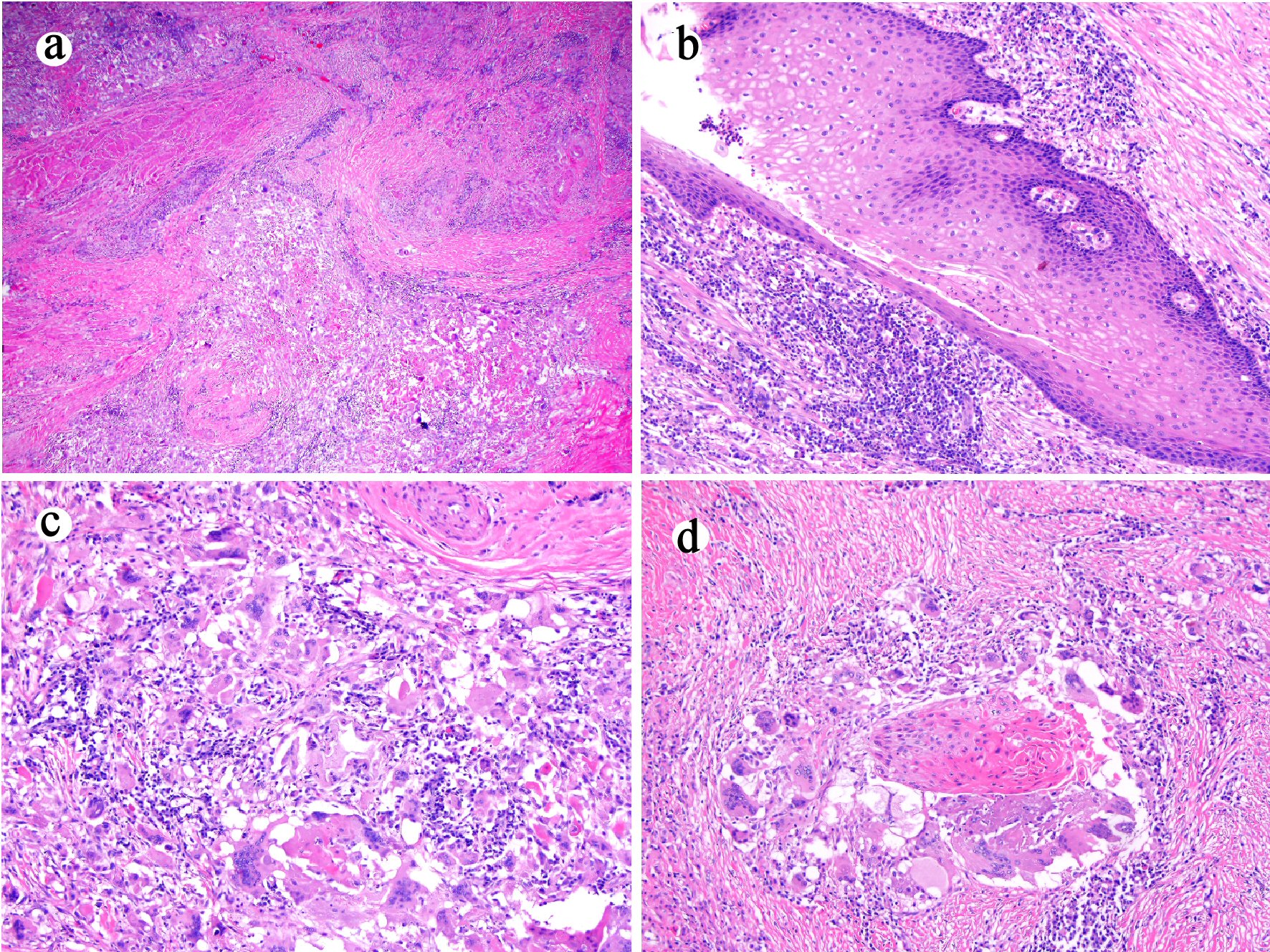
Figure 3. Esophagectomy (case 1) shows mural fibrosis and inflammation ((a) hematoxylin and eosin stain, original magnification × 20), few residual cyst lined with well-differentiated bland squamous epithelium ((b) hematoxylin and eosin stain, original magnification × 100), and histiocytic and giant cell response to keratinous material ((c) hematoxylin and eosin stain, original magnification × 200) and residual squamous carcinomatous cells ((d) hematoxylin and eosin stain, original magnification × 200).
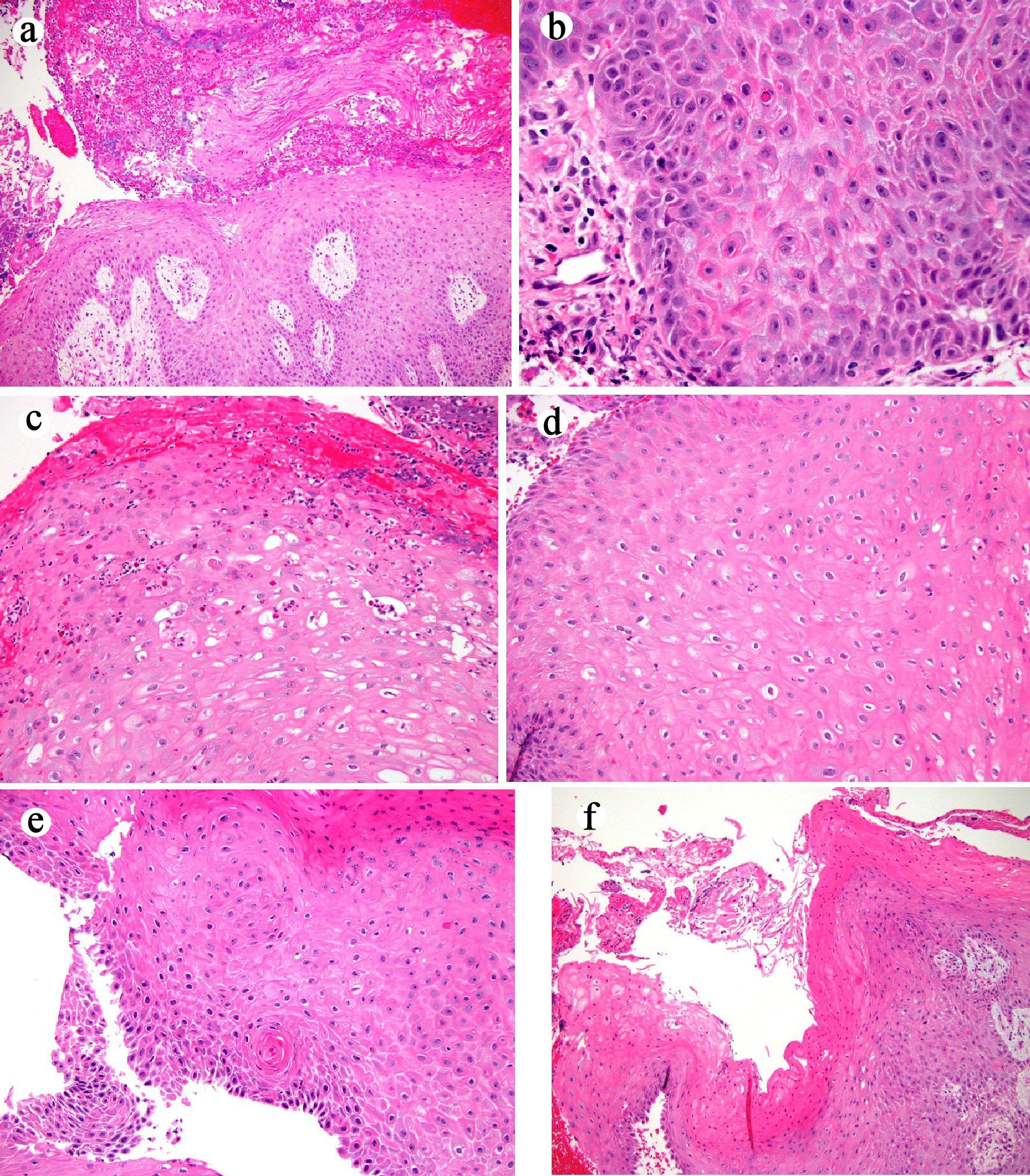
Figure 4. Histologic features of mucosal biopsy from the mass (case 2). Squamous epithelium shows hyperkeratosis and acanthosis ((a) hematoxylin and eosin stain, original magnification × 40), focal atypia ((b) hematoxylin and eosin stain, original magnification × 400), intraepithelial neutrophilic inflammation and microabscesses and dyskeratosis ((c) hematoxylin and eosin stain, original magnification × 200), koilocyte-like cells ((d) hematoxylin and eosin stain, original magnification × 200), deep keratinization ((e) hematoxylin and eosin stain, original magnification × 200), and furrow ((f) hematoxylin and eosin stain, original magnification × 40).
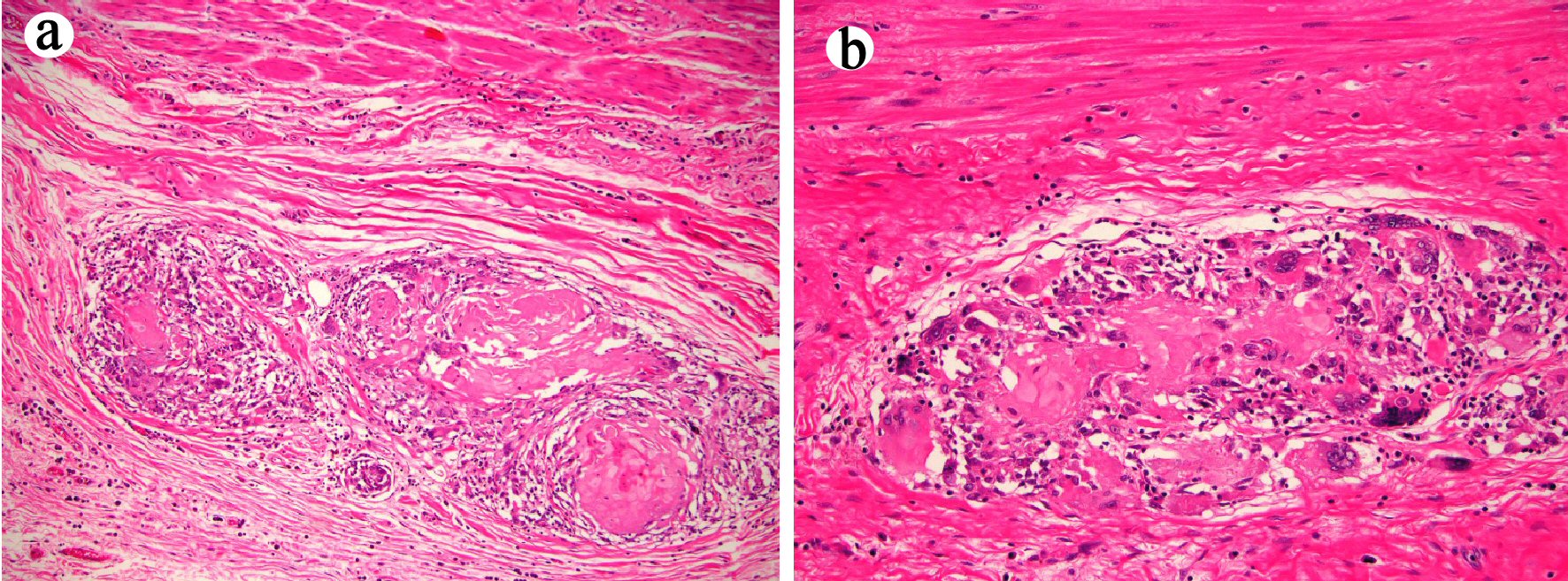
Figure 5. Esophagectomy (case 2) shows histiocytic and giant cell response to keratinous material and residual terminally differentiated squamous carcinomatous cells ((a) and (b) hematoxylin and eosin stain, original magnification × 100 and × 200, respectively).
Tables
Table 1. Clinical, Radiologic, and Endoscopic Findings in These Two Patients With Esophageal Carcinoma Cuniculatum
| Patient | Age | Gender | Symptoms | Chest CT | PET/CT | EGD | EUS |
|---|
| CT: computed tomography; PET/CT: positron emission tomography-computed tomography; EGD: esophagogastroduodenoscopy; EUS: endoscopic ultrasound. |
| 1 | 67 | Male | Progressive dysphagia (4 - 5 months) and 40-lb weight loss | Esophageal wall thickening | Avid esophageal mass (4 cm × 6 cm) | Partially obstructive mass (4 cm) in the distal esophagus and gastroesophageal junction | Hypoechoic mass, extending beyond the muscularis propria and five malignant appearing lymph nodes (EUS staging of T3N2Mx) |
| 2 | 62 | Male | Progressive dysphagia (5 months) and 30-lb weight loss | Esophageal wall thickening | Avid esophageal mass | Firm, friable, partially obstructive and ulcerated mass (4 cm) in the distal esophagus, extending to the cardia | Hypoechoic mass, extending beyond the muscularis propria and one 6 mm hypoechoic lymph node (EUS staging of T3N1Mx) |
Table 2. Histopathologic Findings and Clinical Follow-Up in These Two Patients With Esophageal Carcinoma Cuniculatum
| Patient | Number of biopsy sets | Histology features on biopsy | Preoperative diagnosis | Neoadjuvant treatment | Final histopathologic diagnosis on esophagectomy | Follow-up |
|---|
| 5-FU: 5-fluorouracil. |
| 1 | 2 | Hyperkeratosis, acanthosis, dyskeratosis, deep keratinization, intraepithelial neutrophils, neutrophilic microabscess, focal cytologic atypia, koilocyte-like cells, and keratin-filled cyst/burrows. | Carcinoma cuniculatum | Paclitaxel/carboplatin | Residual carcinoma cuniculatum with marked tumor regression | Patient was well 1 month after esophagectomy. |
| Ulceration |
| Radiation | Mural fibrosis |
| Histiocytic and giant cell response |
| 15 negative lymph nodes |
| ypT3N0Mx |
| 2 | 3 | Hyperkeratosis, acanthosis, dyskeratosis, deep keratinization, intraepithelial neutrophils, neutrophilic microabscess, focal cytologic atypia, koilocyte-like cells, and keratin-filled cyst/burrows. | Carcinoma cuniculatum | 5-FU and cisplatin | Residual carcinoma cuniculatum with marked tumor regression | No recurrence or metastases were detected during his follow-up. Patient died from mixed obstructive-restrictive lung disease 36 months after the esophagectomy. |
| Radiation | Ulceration |
| Mural fibrosis |
| Histiocytic and giant cell response |
| 28 negative lymph nodes |
| ypT3N0Mx |