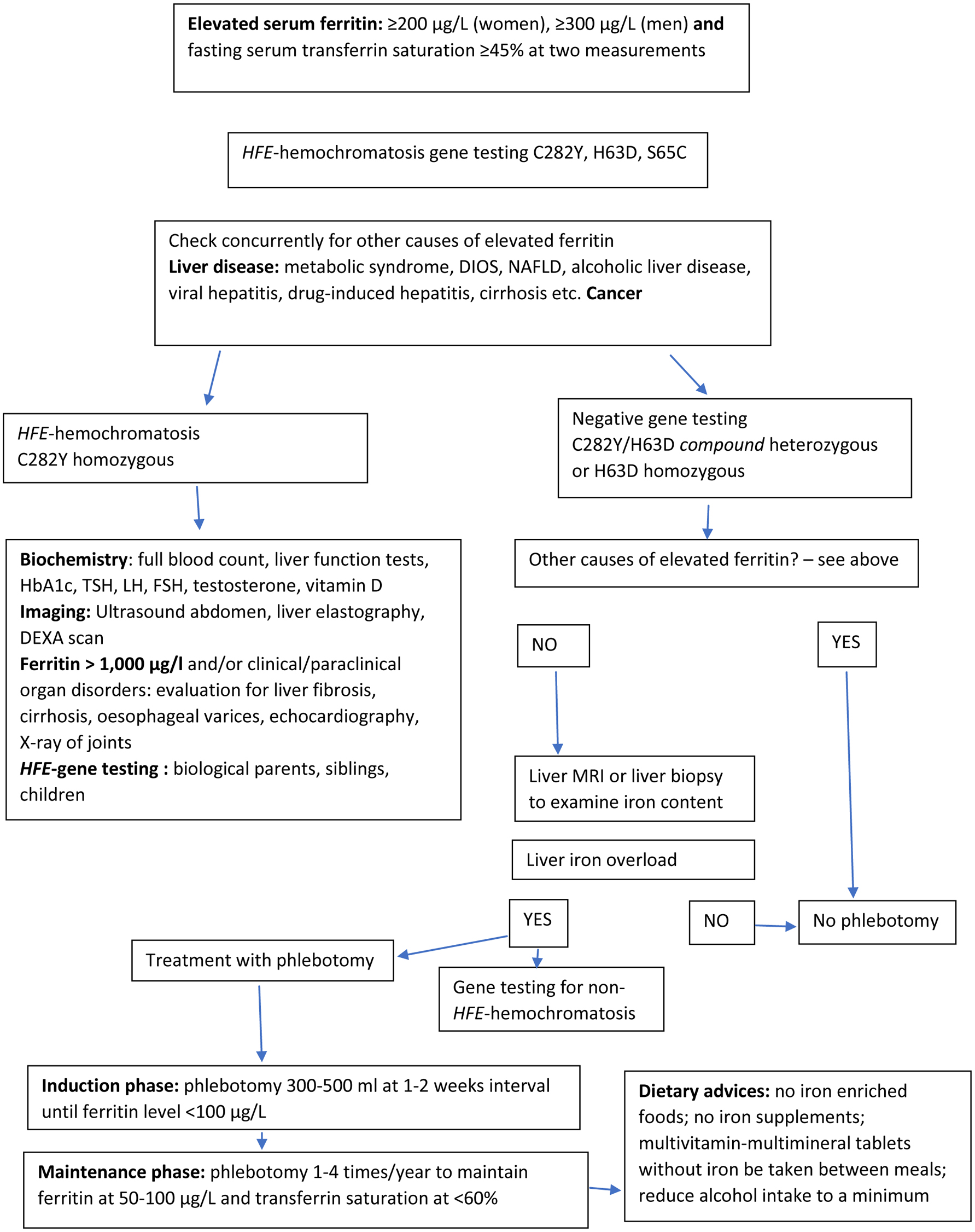
Figure 1. Diagnostic and therapeutic algorithm (simplified) in the assessment of HFE-hemochromatosis.
| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Review
Volume 12, Number 5, October 2019, pages 221-232
Diagnosis and Treatment of Genetic HFE-Hemochromatosis: The Danish Aspect
Figures
Tables
| Checking body iron status (serum ferritin and serum transferrin saturation) in patients with: |
| Persistent fatigue without any obvious explanation |
| Arthralgias, arthritis |
| Elevated biochemical liver tests, liver disease |
| Diabetes mellitus |
| Hypogonadism, erectile dysfunction |
| Cardiac disease |
| Skin pigmentation |
| Induction treatment |
| Phlebotomy 300 - 500 mL at 1 - 2 weeks intervals, until serum ferritin is < 100 µg/L |
| Check hemoglobin before each phlebotomy and ferritin after every fourth phlebotomy |
| Maintenance treatment |
| Phlebotomy 1 - 4 times per year to maintain ferritin level at 50 - 100 µg/L and transferrin saturation < 60% |
| Check hemoglobin, ferritin, and transferrin saturation before and 3 - 4 months after phlebotomy |