Figures
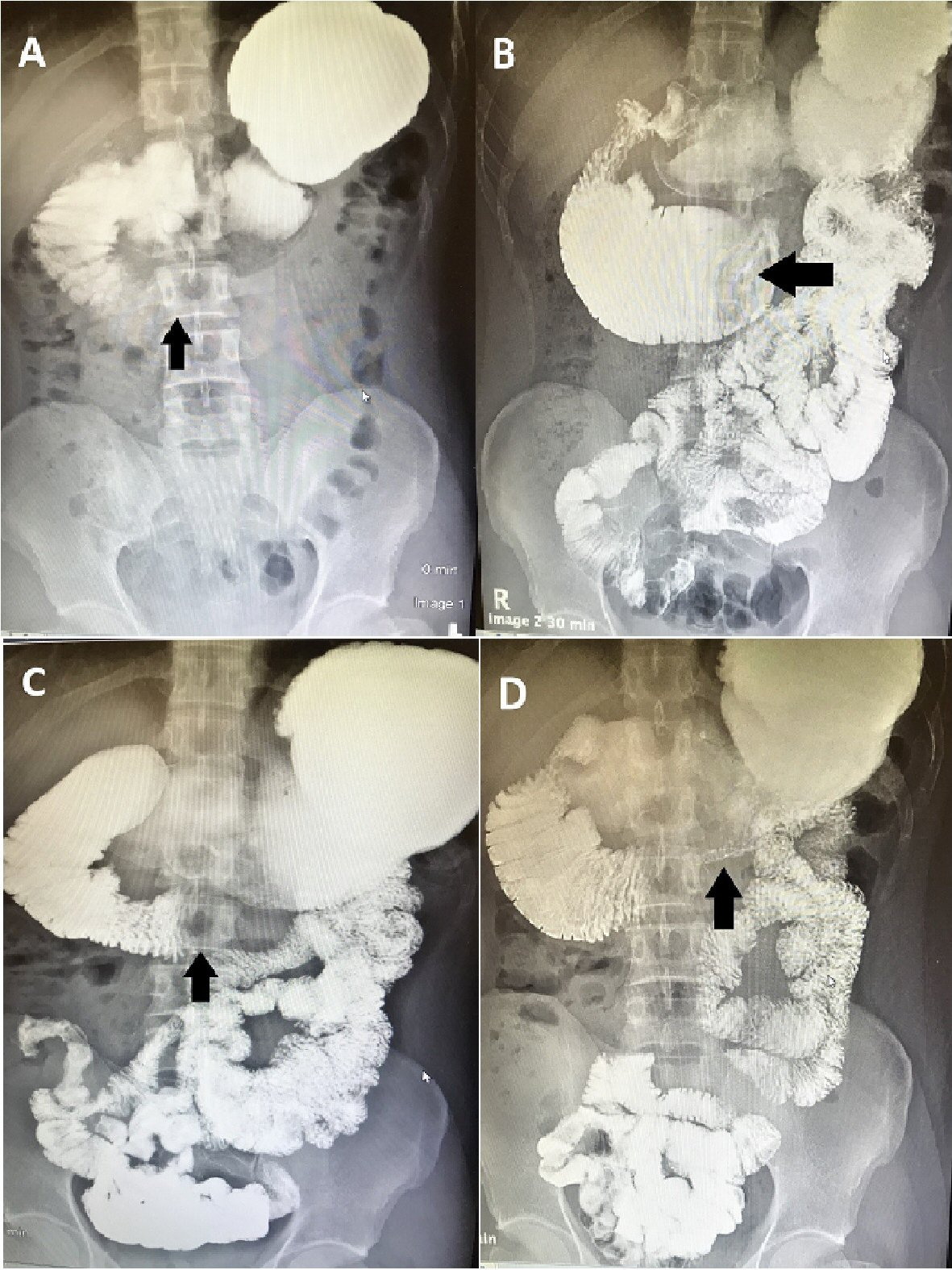
Figure 1. (A-D) Upper gastrointestinal series with small bowel follow-through. Oral contrast was administered. Note the distended stomach and proximal duodenum as well as the narrow distal duodenum. There is abnormal dilation of the third part of the duodenum, measuring 7.1 cm in diameter, as well as delayed passage of contrast into the distal small bowel: features suggestive of a partial distal duodenal obstruction.
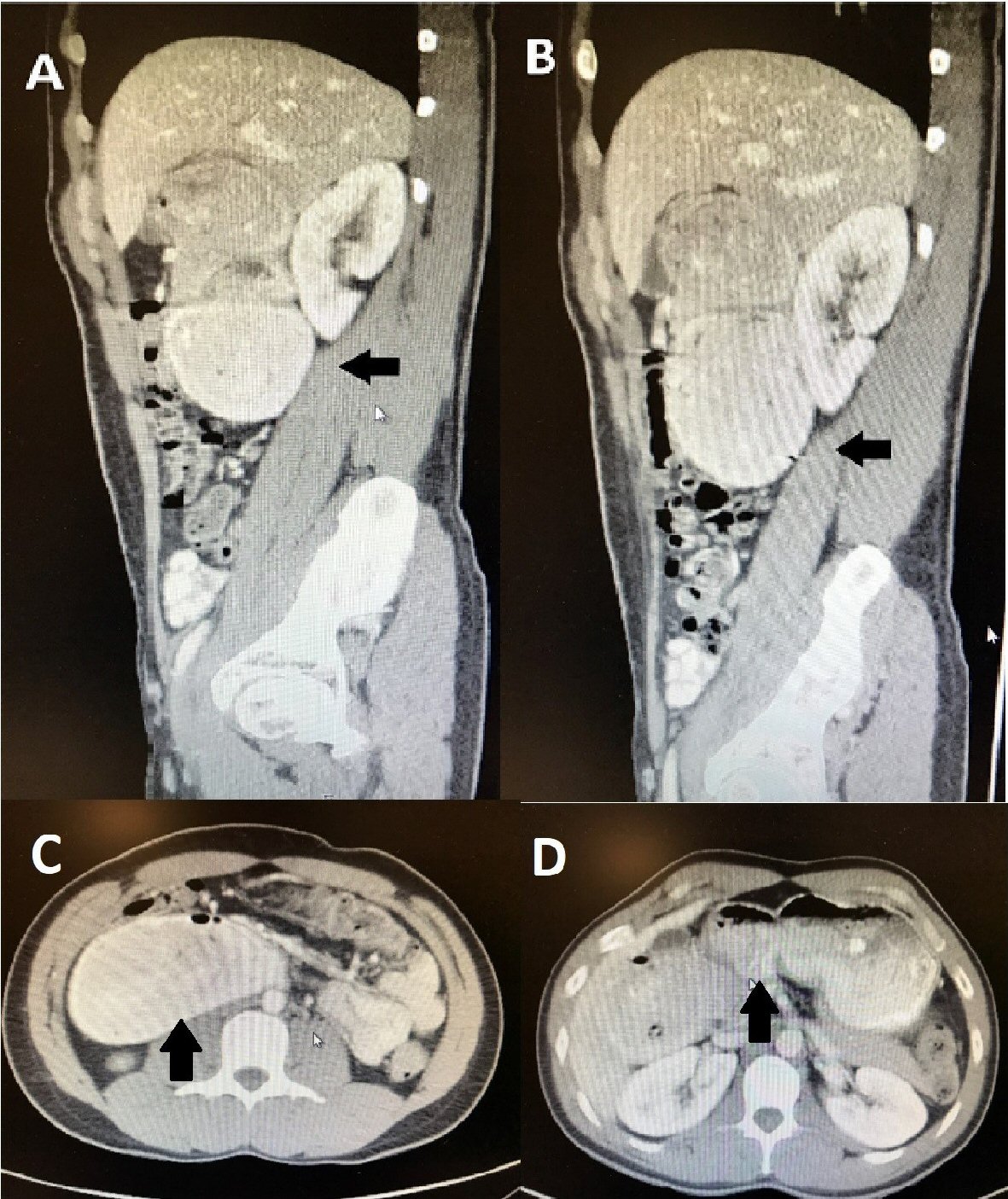
Figure 2. (A-D) Abdominal CT scan. Oral contrast was administered. The patient was discovered to have marked dilation of the second and third parts of the duodenum as well as marked narrowing of the distal third and fourth parts, which was consistent with high-grade partial small bowel obstruction at the distal duodenum.
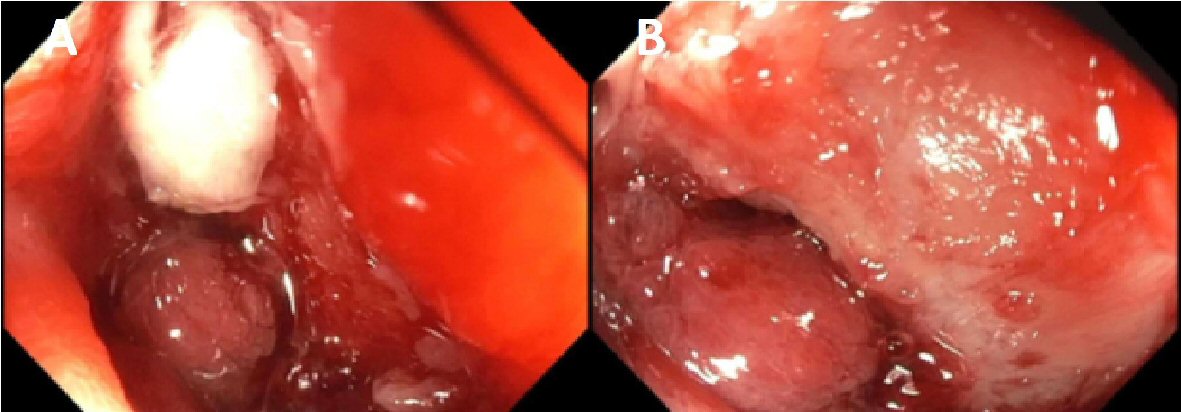
Figure 3. (A, B) Small bowel enteroscopy. A large ulcerated infiltrative mass, with bleeding upon contact and causing mechanical obstruction, was discovered in the fourth part of the duodenum.
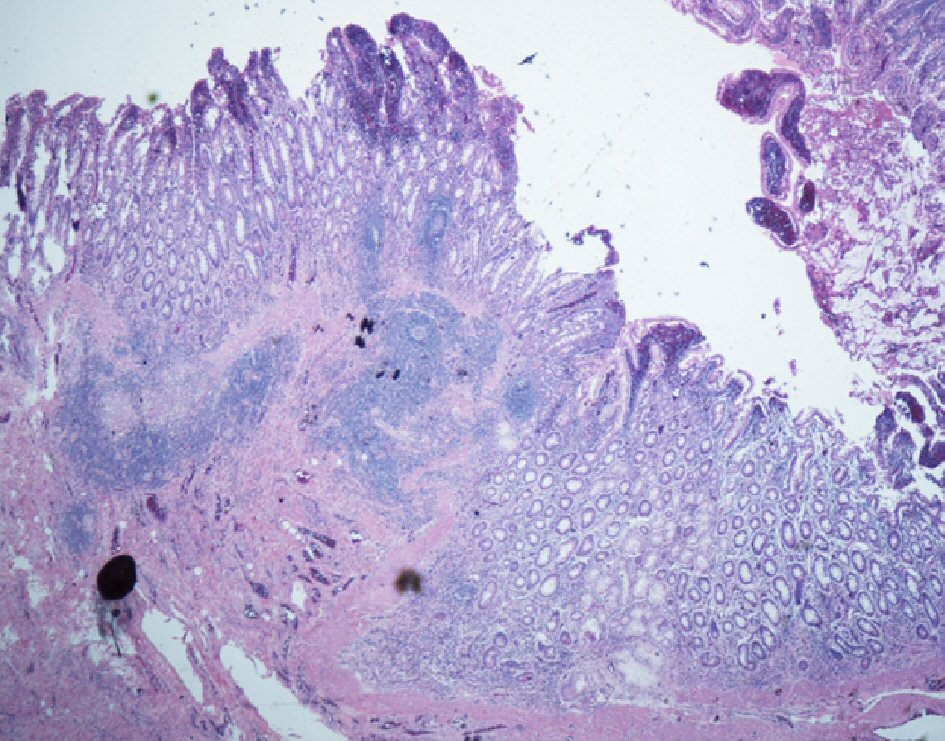
Figure 4. Histopathologic images of the patient’s resected distal duodenum. The duodenal wall shows fissuring mucosal ulcer extending to the submucosa. There are poorly formed non-caseating granulomas. There is transmural inflammation seen in the form of lymphoid aggregates (H&E stain).