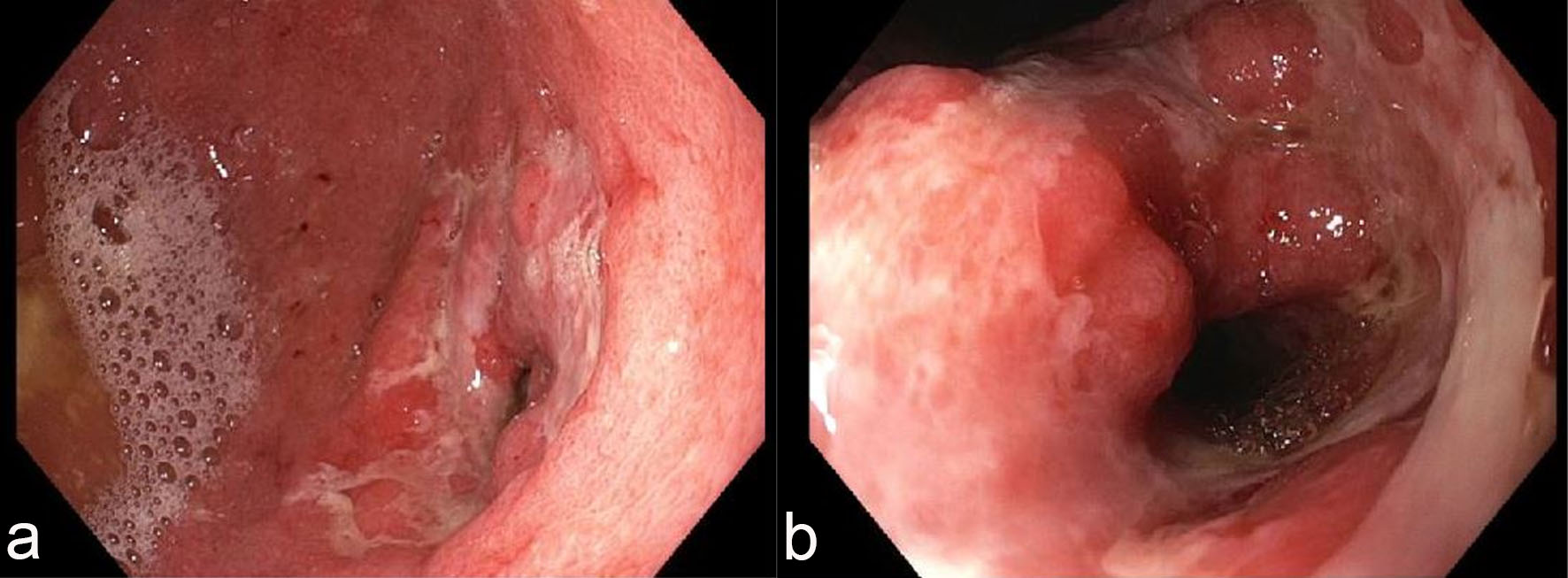
Figure 1. Endoscopic features of the stomach. Esophagogastroduodenoscopy (EGD) revealed diffuse, nodular, erythematous and ulcerated mucosa in the antrum (a) with narrowing of the pyloric channel (b).
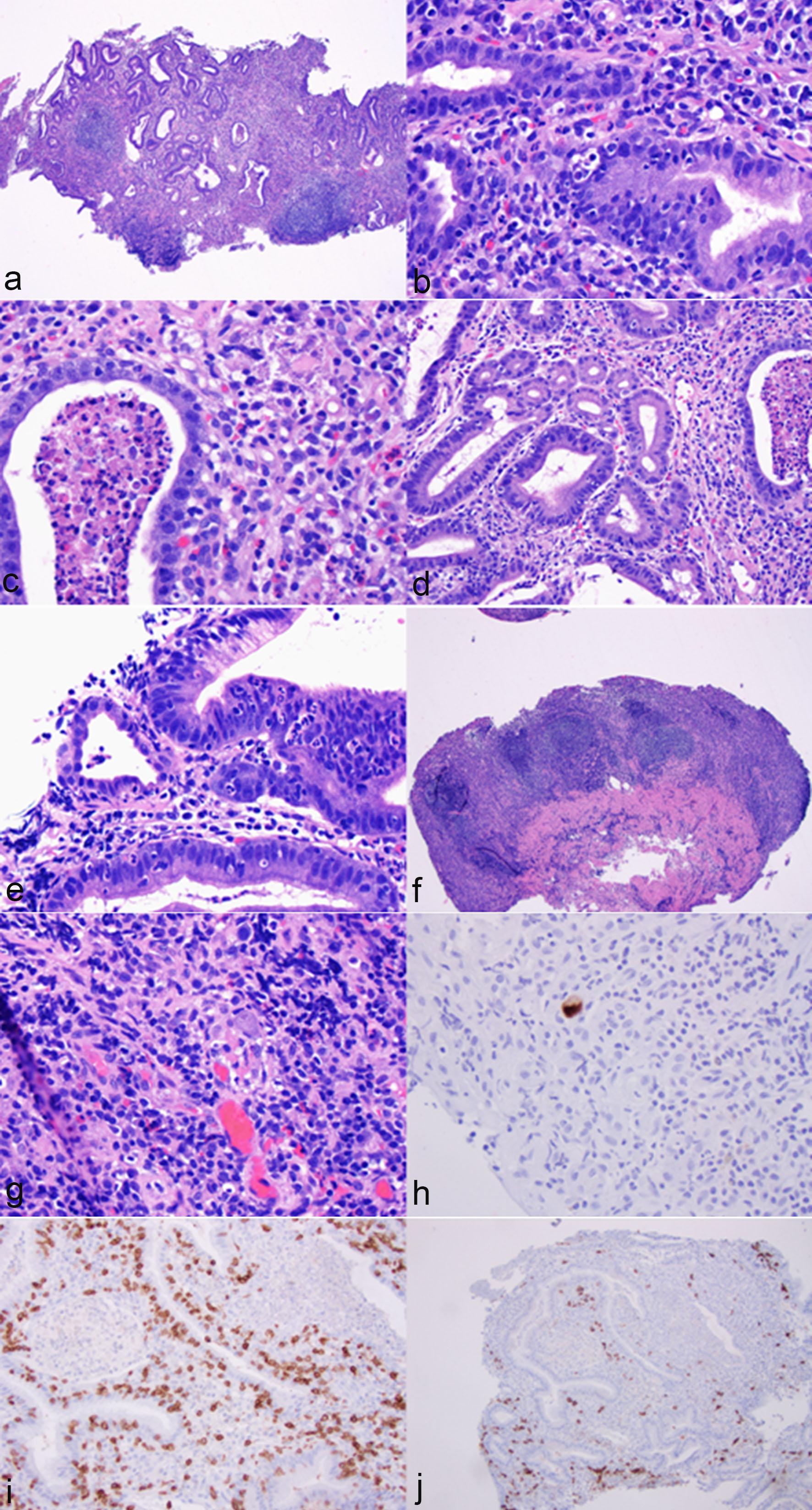
Figure 2. Histological features of immunotherapy-associated gastritis and cytomegaloviral (CMV) infection. The antral mucosa showed marked mononuclear inflammatory cell infiltration in the lamina propria (a, hematoxylin & eosin stain (H&E), ×40), crypt apoptosis (b, H&E stain, ×400), apoptotic abscesses (c, H&E stain, ×400), crypt epithelial lymphocytosis (d, H&E stain, ×200) and neutrophilic infiltration in crypt epithelium (e, H&E stain, ×400). Focal erosion and ulceration were noted (f, H&E stain, ×40). In addition, a few prominent lymphoid aggregates were noted in the lamina propria (f, H&E stain, ×40). The glandular epithelium showed regenerative changes (a). No atypia was noted for lymphocytes (d, f). A few cytomegalovirus-infected cells were noted on routine stain (g, H&E stain, ×400) and confirmed by immunohistochemistry (h, immunoperoxidase stain, ×400). Immunohistochemistry for CD3 and CD20 revealed a mixed population of T cells and B cells with T cells primarily in the crypt epithelium and B cells in the lamina propria (i, immunoperoxidase stain, ×200; j, immunoperoxidase stain, ×100).