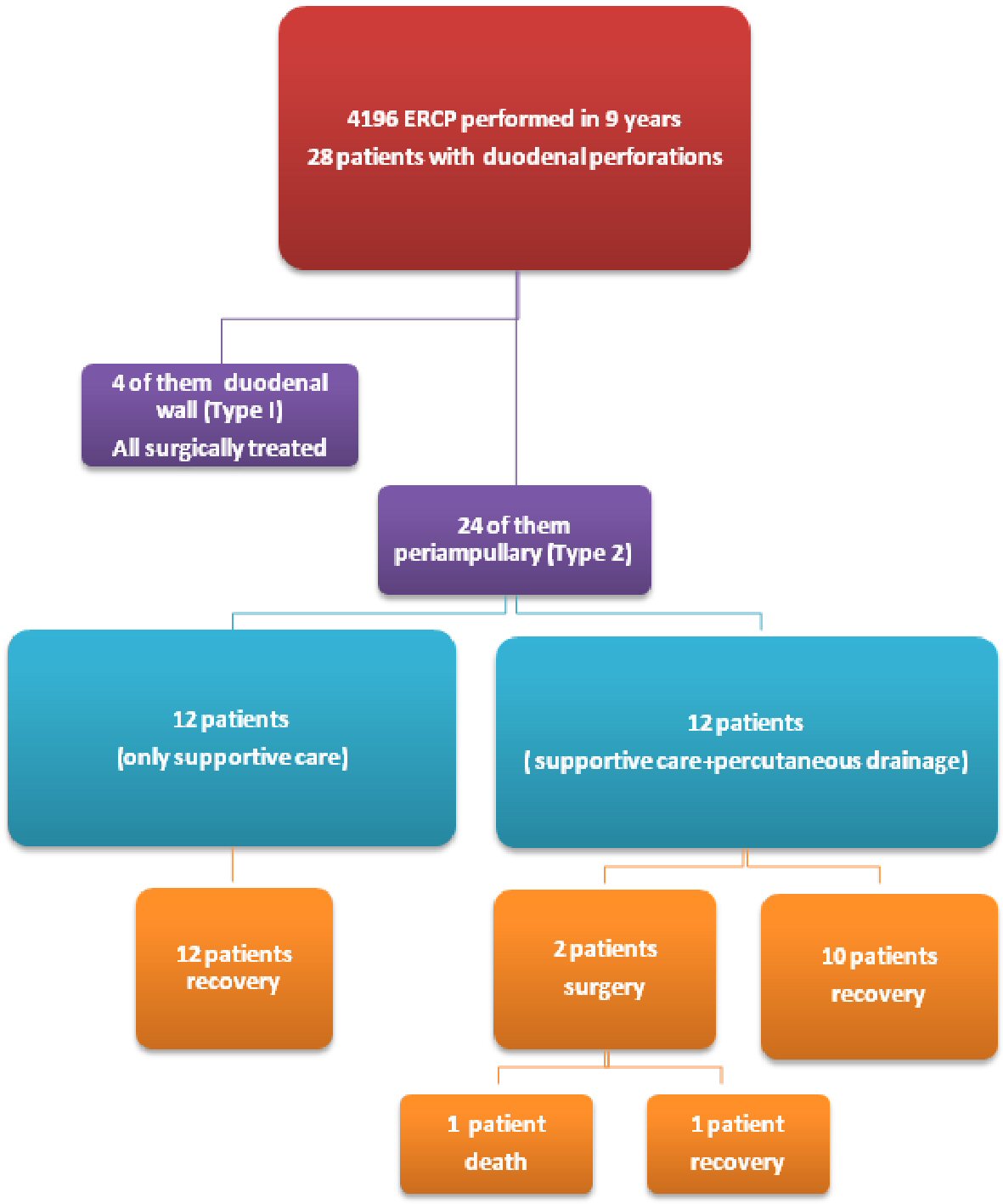
Figure 1. Flow-chart for clinical outcome of 24 patients with post-ERCP type 2 perforations.
| Gastroenterology Research, ISSN 1918-2805 print, 1918-2813 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Gastroenterol Res and Elmer Press Inc |
| Journal website http://www.gastrores.org |
Original Article
Volume 11, Number 3, June 2018, pages 207-212
Non-Operative Management of Type 2 ERCP-Related Retroperitoneal Duodenal Perforations: A 9-Year Experience From a Single Center
Figures
Tables
| Characteristics | Value (%) |
|---|---|
| Age, year | |
| Mean (SD) | 71.3 ± 17.1(16.7) |
| Range | 24 - 90 |
| Median | 71.1 |
| Gender | |
| Male | 10 (41.7) |
| Female | 14 (58.3) |
| ERCP indication | |
| Obstructive jaundice | 3 (12.5) |
| Choledocholithiasis | 20 (83.4) |
| Ampullectomy | 1 (4.1) |
| Type of procedure | |
| Guidewire-assisted sphincterotomy | 19 (79.2) |
| Needle-knife precut sphincterotomy | 3 (12.5) |
| Large balloon dilatation | 1 (4.2) |
| Ampullectomy | 1 (4.2) |
| Conservative only treatment (n = 12) | Conservative only treatment + CT-guided percutaneous drainage (n = 12) | |
|---|---|---|
| Attempted endoscopic closure | 1 FCSEMS | 1 Endoclips |
| Hospitalization time | 10.0 ± 2.4 (range 7 - 14) days | 13.1 ± 10.8 (range 7 - 45) days |
| Total parental nutrition | 0 | 4 (33.4%) |
| Surgery | 0 | 2 (16.6%) |
| Death | 0 | 1 (8.3%) |